Some Americans have refused, wrongly claiming mask decrees violate the Constitution. An internet search turns up dozens of examples.
“Costco Karen,” for instance, staged a sit-in in a Costco entrance in Hillsboro, Oregon after she refused to wear a mask, yelling “I am an American … I have rights.”
A group called Health Freedom Idaho organized a protest against a Boise, Idaho, mask mandate. One protester said, “I’m afraid where this country is headed if we just all roll over and abide by control that goes against our constitutional rights.”
As one protester said, “The coronavirus doesn’t override the Constitution.”
Speaking as a constitutional law scholar, these objections are nonsense.
The objections
It is not always clear why anti-maskers think government orders requiring face coverings in public spaces or those put in place by private businesses violate their constitutional rights, much less what they think those rights are. But most of the mistaken objections fall into two categories:
Mandatory masks violate the First Amendment right to speech, assembly, and especially association and mandatory masks violate a person’s constitutional right to liberty and to make decisions about their own health and bodily integrity.
They’re not mutually exclusive claims: A lawsuit filed by four Florida residents against Palm Beach County, for example, argued that mask mandates “interfere with … personal liberty and constitutional rights,” such as freedom of speech, right to privacy, due process, and the “constitutionally protected right to enjoy and defend life and liberty.” The lawsuit asked the court to issue a permanent injunction against the county’s mask mandate.
On July 27, the Court declined to issue an injunction against the mask mandate. Citing Jacobsen v. Massachusetts, the Court found that “no constitutional right is infringed by the Mask Ordinance’s mandate … and that the requirement to swear such a covering has a clear rational basis based on the protection of public health.” More to the point, the Court continued, “constitutional rights and the ideals of limited government do not … allow (citizens) to wholly shirk their social obligation to their fellow Americans or to society as a whole…. After all, we do not have a constitutional right to infect others.”
Responding to a reporter who asked why President Donald Trump appeared unconcerned about the absence of masks and social distancing at a campaign rally in Tulsa, Vice President Mike Pence said: “I want to remind you again freedom of speech and the right to peaceably assemble is in the Constitution of the U.S. Even in a health crisis, the American people don’t forfeit our constitutional rights.”
What the First Amendment does – and doesn’t – do
The First Amendment protects freedom of speech, press, petition, assembly and religion.
There are two reasons why mask mandates don’t violate the First Amendment.
First, a mask doesn’t keep you from expressing yourself. At most, it limits where and how you can speak. Constitutional law scholars and judges call these “time, place, and manner” restrictions. If they do not discriminate on the basis of the content of the speech, such restrictions do not violate the First Amendment. An example of a valid time, place and manner restriction would be a law that limits political campaigning within a certain distance of a voting booth.
Additionally, the First Amendment, like all liberties ensured by the Constitution, is not absolute.
All constitutional rights are subject to the goverment’s authority to protect the health, safety and welfare of the community. This authority is called the “police power.” The Supreme Court has long held that protecting public health is sufficient reason to institute measures that might otherwise violate the First Amendment or other provisions in the Bill of Rights. In 1944, in the case of Prince v. Massachusetts, for example, the Supreme Court upheld a law that prohibited parents from using their children to distribute religious pamphlets on public streets.
A man protesting a mask mandate in Florida says he’s standing up for “the rights of people to make their own medical decisions.”
The right to liberty
Some anti-maskers object that masks violate the right to liberty.
The right to liberty, including the right to make choices about one’s health and body, is essentially a constitutional principle of individual autonomy, neatly summarized as “My body, my choice.”
The 1905 case of Jacobsen v. Massachusetts shows why mask mandates don’t violate any constitutional right to privacy or health or bodily integrity. In that case, the Supreme Court upheld a smallpox vaccination requirement in Cambridge, Massachusetts.
The court said that the vaccination requirement did not violate Jacobsen’s right to liberty or “the inherent right of every freeman to care for his own body and health in such way as to him seems best.”
As the court wrote, “There are manifold restraints to which every person is necessarily subject for the common good. On any other basis, organized society could not exist with safety to its members.” In a 1995 New York case, a state court held that an individual with active tuberculosis could be forcibly detained in a hospital for appropriate medical treatment.
Even if you assume that mask mandates infringe upon what the Supreme Court calls “fundamental rights,” or rights that the court has called the “very essence of a scheme of ordered liberty,” it has consistently ruled states can act if the restrictions advance a compelling state interest and do so in the least restrictive manner.
Rights are conditional
As the Jacobsen ruling and the doctrine of time, place and manner make clear, the protection of all constitutional liberties rides upon certain necessary – but rarely examined – assumptions about communal and public life.
One is that constitutional rights – whether to liberty, speech, assembly, freedom of movement or autonomy – are held on several conditions. The most basic and important of these conditions is that our exercise of rights must not endanger others (and in so doing violate their rights) or the public welfare. This is simply another version of the police power doctrine.
Unfortunately, a global pandemic in which a serious and deadly communicable disease can be transmitted by asymptomatic carriers upsets that background and justifies a wide range of reasonable restrictions on our liberties. Believing otherwise makes the Constitution a suicide pact – and not just metaphorically.
This story has been updated to reflect a ruling in the Palm Beach County court challenge to a mask mandate.
Here’s some advice for frustrated impeachment advocates who think there might be other ways to force Donald Trump out of office: The 25th Amendment won’t help you.
In an interview with “60 Minutes,” McCabe claimed that people in the Department of Justice, including Deputy Attorney General Rod Rosenstein and McCabe himself, had discussed trying to get a majority of the Cabinet to agree to remove Donald Trump from office. (Rosenstein denied the story, but it didn’t go away.)
If that majority vote is all the amendment requires, it would provide a much easier process than impeachment to dump a president.
‘Doomed to failure’
Writing in The Wall Street Journal, prominent conservative lawyers David B. Rivkin and Lee A. Casey wrote that, if those DOJ discussions in fact took place and were serious, the participants were part of “a conspiracy by government officials against American democracy.”
That sounds awful, but any such technical conspiracy – if that’s what it was – was doomed to failure.
If the DOJ lawyers thought getting rid of a president – this one or a future holder of the office – was easy, they hadn’t studied the amendment’s language.
I’m a professor of law – a tax professor at that. I’m used to parsing difficult legal language, and I’ve written about constitutional issues as well as ones that arise in bean-counting. The 25th Amendment is a complex law that is, by design, very hard to use.
Roots in Kennedy assassination
A little history: The 25th amendment was ratified in 1967. A primary purpose was to provide a way to fill the vice presidency when that office becomes vacant.
The first, the easy case, is when the president himself sends a written declaration to the speaker of the House and the president of the Senate that “he is unable to discharge the powers and duties of his office.”
The president says, in effect, “I can’t handle the job right now, but I’ll be back.”
The vice president steps in temporarily, and the president reassumes presidential duties when he notifies congressional leaders that he’s up to it.
But the rules applicable to the other situation in which a vice president can become acting president are much less clear.
Somehow the idea got around – reflected in the alleged DOJ discussions – that, if some officials think a president is incapacitated, but he disagrees or is so out of it that he can’t voluntarily step aside, a majority of the Cabinet can promote the vice president.
I believe that understanding is wrong.
To begin with, under the 25th Amendment it’s “the Vice President and a majority of either the principal officers of the executive departments or such other body as Congress may by law provide” who must make the declaration of incapacity to congressional officers.
If Vice President Pence sides with the president – as I believe he would unless Trump were clearly incapacitated – it doesn’t matter what Cabinet officials think.
And “principal officers of the executive departments” doesn’t necessarily mean the Cabinet, although it could. “Cabinet” isn’t a constitutional term.
It’s up to the president who sits in his Cabinet, or, for that matter, whether the Cabinet sits at all. Not everyone in the Trump Cabinet is a principal officer of an executive department: the U.N. ambassador and White House chief of staff, for example. And many people who head federal agencies, and who therefore might be treated as “principal officers of executive departments,” aren’t in the Cabinet – like the secretary of the Navy.
It’s hard to determine whether there’s a majority of principal officers on board if it’s not clear who gets counted for this purpose. Besides, the president could change the numbers by firing principal officers, whoever they might be, if he learns that a revolt is brewing.
Congress unlikely to act
The amendment does permit Congress to provide for an alternative body that can, with the agreement of the vice president, make an initial determination of presidential incapacity.
It would be nice if Congress had done this at some point in the past 50-some years, to provide more certainty about what should happen when a president is incapacitated. But I believe Congress is unlikely to act under the 25th Amendment until political tensions have eased – whenever that might be – and a different president is in office.
In any event, even if there were no computational difficulties, and even if the vice president were to agree that the president is incapacitated, the amendment doesn’t provide for actually removing the president from office.
Furthermore, a deposed president can return to power.
Under the amendment, once the president declares “that no inability exists,” he resumes presidential duties, unless the acting president and a majority of principal officers – that phrase again! – disagree and Congress, by a two-thirds vote of both houses, also disagrees.
Alabama’s governor signed a bill this week that criminalizes nearly all abortions, threatening providers with a felony conviction and up to 99 years in prison.
It is one of numerous efforts across the United States to restrict access to abortion and challenge the Supreme Court’s 1973 decision in Roe v. Wade that legalized abortion nationwide.
Six states have recently passed legislation that limit abortions to approximately six weeks after the end of a woman’s last period, before many know they are pregnant. Although the laws have not yet taken effect and several have been blocked on constitutional grounds, if enacted they would prohibit most abortions once a doctor can hear rhythmic electrical impulses in the developing fetus.
Called “fetal heartbeat” bills, they generally refer to the fetus as an “unborn human individual.” It is a strategic choice, trying to establish fetal personhood, but it also reveals assumptions about human life beginning at conception that are based on particular Christian teachings.
Not all Christians agree, and diverse religious traditions have a great deal to say about this question that gets lost in the polarized “pro-life” or “pro-choice” debate. As an advocate of reproductive rights, I have taken a side. Yet as a scholar of Jewish Studies, I appreciate how rabbinic sources grapple with the complexity of the issue and offer multiple perspectives.
What Jewish texts say
Traditional Jewish practice is based on careful reading of biblical and rabbinic teachings. The process yields “halakha,” generally translated as “Jewish law” but deriving from the Hebrew root for walking a path.
Even though many Jews do not feel bound by “halakha,” the value it attaches to ongoing study and reasoned argument fundamentally shapes Jewish thought.
Although the Hebrew Bible does not mention abortion, it does talk about miscarriage in Exodus 21:22-25. It imagines the case of men fighting, injuring a pregnant woman in the process. If she miscarries but suffers no additional injury, the penalty is a fine.
Since the death of a person would be murder or manslaughter, and carry a different penalty, most rabbinic sources deduce from these verses that a fetus has a different status.
An early, authoritative rabbinic work, the Mishnah, discusses the question of a woman in distress during labor. If her life is at risk, the fetus must be destroyed to save her. Once its head starts to emerge from the birth canal, however, it becomes a human life, or “nefesh.” At that point, according to Jewish law, one must try to save both mother and child. It prohibits setting aside one life for the sake of another.
Although this passage reinforces the idea that a fetus is not yet a human life, some orthodox authorities allow abortion only when the mother’s life is at risk.
Other Jewish scholars point to a different Mishnah passage that envisions the case of a pregnant woman sentenced to death. The execution would not be delayed unless she has already gone into labor.
Jewish sources generally see the fetus as part of the mother.
In the Talmud, an extensive collection of teachings building on the Mishnah, the rabbis suggest that the ruling is obvious: the fetus is part of her body. It also records an opinion that the fetus should be aborted before the sentence is carried out, so that the woman does not suffer further shame.
Later commentators mention partial discharge of the fetus brought on by the execution as an example – but the passage’s focus on the needs of the mother can also broaden the circumstances for allowing abortion.
Making space for divergent opinions
These teachings represent only a small fraction of Jewish interpretations. To discover “what Judaism says” about abortion, the standard approach is to study a variety of contrasting texts that explore diverse perspectives.
Over the centuries, rabbis have addressed cases related to potentially deformed fetuses, pregnancy as the result of rape or adultery, and other heart-wrenching decisions that women and families have faced.
In contemporary Jewish debate there are stringent opinions adopting the attitude that abortion is homicide – thus permissible only to save the mother’s life. And there are other lenient interpretations broadly expanding justifications based on women’s well-being.
Yet the former usually cite contrary opinions, or even refer a questioner to inquire elsewhere. The latter still emphasize Judaism’s profound reverence for life.
According to the 2017 Pew survey, 83% of American Jews believe that abortion should be legal in all or most cases. All the non-orthodox movements have statements supporting reproductive rights, and even ultra-orthodox leaders have resisted anti-abortion measures that do not allow religious exceptions.
An academic expert on Islamophobia attended a ‘free-speech’ conference in Toronto, where she was assaulted after challenging speakers for promoting hatred against Muslims.
The horror of the New Zealand terror attack that targeted two mosques during Friday congregational prayers and left 50 people dead has raised important questions about the kind of ideas that inspire this senseless violence. In Canada, the 2017 Québec mosque shooting that left six Muslim men dead also forced the question: what drives the hate that leads to white nationalist terror?
Recently I attended a “free speech” conference on the outskirts of Toronto. In attendance at the event were lawyers from prominent legal firms and other professionals. When I challenged one of the speakers for remarks I felt promoted hatred against Muslims, I was physically assaulted.
I have long been examining the question of what fuels white nationalist hatred by documenting and mapping the “Islamophobia industry” in Canada. The industry is a constellation of individuals, media outlets, think tanks, politicians and organizations that purvey racism and Islamophobia. These include white nationalist and “alt-right” groups that are proliferating and expanding their reach in Canada from upward of 100 groups in 2015 to nearly 300 by 2018.
While the alt-right, neo-Nazi and white supremacist groups are the foot soldiers of the movement, there are other, more covert players that form the soft power of this widespread industry. These power brokers use cultural, political and economic ideas to influence, shape and inform white nationalist views. They help circulate bigotry by dressing it up as patriotism and purveying it through “respectable” channels.
I refer to this as the “liberal washing” of white nationalism, where politically camouflaged xenophobic, Islamophobic and racist notions are disguised under the veneer of liberal discourse such as “protecting democracy,” “freedom” and the “rule of law” from what are regarded as illiberal, anti-modern and anti-democratic minorities.
I had a front-row seat to liberal-washed hate messaging at the conference held by Canadians for the Rule of Law, a registered charity that seeks to challenge “political tribes” and “disruptors” who question the rule of law in Canada.
Teaching Islamophobic fear and bigotry
The idea that “Islamists” are infiltrating and imposing shariah law in Canada was a common narrative at this event and disturbingly echoed the views of the New Zealand shooter, whose manifesto spoke of Muslim “invaders” who were corrupting western civilization.
Protesters decrying hatred and racism converged around the U.S. after a white supremacist rally that spiraled into deadly violence in Virginia in the summer of 2017.
(Anna Reed/Statesman-Journal/AP)
The vague deployment of the term “Islamist” at this conference reduced a broad political spectrum to a narrow epithet for the violent overthrow of democratic rule to install an Islamic State. The Islamist bogeyman became the dominant representation of Muslims. Fear-mongering about the infiltration of the Muslim Brotherhood in Canada was used as a clarion call to warn of impending threats to Canada’s freedom and democracy from Muslim neighbours, organizations, politicians, Muslim Student Associations and Islamic schools.
Preserving Canadian “values” from the corruption of minorities seems far more reasonable than shouting racist slogans in the street — except this liberal-washing of hate is simply another way of echoing and dog-whistling white nationalist, xenophobic ideals by masquerading them through more “civil” and “polite” discourse.
One of the supporting organizations of the conference was Act For Canada, an offshoot of Act For America, one of the most prominent anti-Muslim groups in the United States. Their website outlines their goals:
“ACT! For Canada is a forum for citizens concerned about the triumphalist brand of Islam that seeks to erode our cherished western principles of free speech and equality with the goal of eventual Islamic supremacy in the West ….”
Other groups supporting the conference included conservative media outlet TAG TV, the Bangladeshi Minority Rights group, B’nai Brith and several pro-Zionist groups that equate criticism of Israel as anti-Semitic and “illegal.” The conference also received funding from Daniel Pipe’s Middle East Forum think tank that “protects western values from Middle Eastern threats” and “emphasizes the danger of lawful Islamism.”
A front row seat to hate
To set the tone for the day, conference organizers began with a condemnation of the New Zealand terror attack. Attendees were asked to rise for a moment of silence. It turns out the silence was not to commemorate the victims of this heinous hate crime, but rather to honour “free speech.”
I spent a long day of being a fly on the wall at this conference, hearing non-stop pro-Zionist rhetoric denying that Israel was oppressing Palestinians and consuming a steady diet of Islamophobic bigotry. Along with this came calls for preserving “Judeo-Christian democracy,” protecting against multiculturalism and the need to build a “coalition of the willing,” (the term used by George W. Bush to refer to countries who supported militarily or politically the 2003 U.S-led invasion of Iraq), to challenge “Islamists” and preserve the rule of law in Canada.
Most egregiously, in one session I attended, panellists repeatedly referred to the Al Noor mosque in New Zealand where the terror attack occurred as a “known site of radicalization” without citing any evidence. They complained the media was not publicizing this information. Despite their caution to say this was not a justification for the shootings, I was concerned their salacious and unfounded claim against the Al Noor mosque created further fear and hatred against Muslims.
Mourners pay their respects at a makeshift memorial near the Masjid Al Noor mosque in Christchurch, New Zealand, on March 16, 2019, after a 28-year-old white supremacist was accused in mass shootings at the mosque that left 50 people dead.
“Islamic supremacists will smile at you and invite you to their gatherings, make you feel loved and welcomed but they do it to deceive you and take over you, your land, and your freedoms …Many friendly, seemingly ‘moderate’ Muslims are deceiving you …”
I asked her what her warning was for Canadians, given that’s what she told Icelanders.
Not so free speech
Douglass-Williams became defensive and said she was misquoted. I was paraphrasing, but I told her I took the information directly from an article she wrote. The moderator became angry and told me I couldn’t speak anymore. He told me to leave.
I protested and said I was trying to engage in a dialogue, to exercise my free speech rights, which this conference purported to uphold. The moderator, who is an “ethicist,” informed me I was now trespassing and had to leave.
Did I breach conference decorum by being unwilling to be silenced? Yes. Did they have a right to ask me to leave because I spoke after being told to be quiet? Technically, yes. I did not plan to interrupt the far-right echo chamber, but when I did intervene in the discussion, I realized it was likely I’d be asked to leave because of my views. And I was willing to do so peacefully. But I was not prepared for what happened next.
I stood up voluntarily to leave as instructed by the moderator. But I made one final comment: I said their thinly veiled white supremacist views and Islamophobic fear-mongering is the kind of rhetoric that inspires white nationalist terror.
That comment caused a commotion.
A man from the audience grabbed me and pulled me from the room, twisting my arm with force. I shouted to the silent onlookers: “This man is hurting me! He has no right to touch me!”
A man in the audience shouted back: “You are lucky to even be in this country!”
During this incident, not one person said or did anything. All cellphones, by order of the conference, were surrendered so no one took videos of the incident. I had to wait to call the police until afterwards.
As the man was physically accosting me, I looked over my shoulder to the crowd in the room. They did not look like Proud Boys wearing Doc Martens; they were mainly white seniors that included a retired school psychologist, a teacher and lawyers dressed in suits and ties. Others wore leisurewear, the kind worn on a winter cruise.
One of the people in the room was a former Toronto police officer and “security expert.” I thought he might see the danger in the situation and stop it, so I appealed to him: “You are a former police officer and I’m telling you this man is assaulting and hurting me!”
He stared at me and said nothing. Ironically, all of this occurred during a panel about public safety and upholding “the rule of law.” No amount of “liberal washing” will clean this dirty laundry.
Editor’s Note: Prior to publishing this article, The Conversation Canada asked the organizer of the conference, Canadians for the Rule of Law, why Jasmin Zine was forcibly removed from the event she attended. Donald Carr, president of Canadians for the Rule of Law, replied in an email that Zine “did not conform to clearly stated ‘rules’ relating to asking questions of the panellists.” Carr said Zine was asked to surrender the microphone after asking her question and that conference organizers then considered her to be a “trespasser on private property” and asked the conference’s private security firm to escort her out. Carr admitted an “unknown individual from the audience seized the professor to take her out, but on request, released her” and a security officer escorted Zine to the lobby of the building. Carr said a police officer subsequently interviewed several people and told conference staff that there “had been no illegal action.” Zine has since received an email from the investigating officer from York Regional Police who indicated that people at the conference he spoke to “were not very forthcoming with information about the suspect.” The officer said conference organizers told him the suspect was selling books at the conference, but they didn’t have any contact information for him. “I’m sorry I could not find the suspect and give you anymore closure in this upsetting matter,” the officer concluded.
When lives are tragically cut short, it is generally easier to explain the “how” than the “why”. This dark reality is all the more felt when tragedy comes at the hands of murderous intent. Explaining how 50 people came to be killed, and almost as many badly injured, in Christchurch’s double massacre of Muslims at prayer is heartbreaking but relatively straightforward.
As with so many mass murders in recent years, the use of an assault rifle, the ubiquitous AR15, oxymoronically referred to as “the civilian M-16”, explains how one cowardly killer could be so lethal.
It is a credit to the peaceful nature of New Zealand society that, despite the open availability of weapons like the AR15, the last time there was a mass shooting was in 1997. Prime Minister Jacinda Ardern rightly identified reform of gun laws as one of the immediate outcomes required in response to this tragedy.
But lax gun laws are arguably the only area in which blame can be laid in New Zealand. Ardern, together with Australian Prime Minister Scott Morrison, was also right to refer to this barbaric act of cold-blooded murder of people in prayer as right wing extremist terrorism driven by Islamophobic hatred.
State and federal police in Australia have long warned that, next to the immediate threat posed by Salafi jihadi terrorism, they are most concerned about the steady rise of right-wing extremism. There has been some comfort in the recognition that the most active right wing extremist groups, and there are many, are disorganised, poorly led, and attract but small crowds.
On the face of it, then, right wing extremism in Australia is nowhere near as serious as the neo-Nazi movements of Europe or the various permutations of white supremacy and toxic nationalism that bedevil American politics. In America, it is conservatively estimated that there were 50 deaths due to terrorist attacks in 2018, almost all linked to right-wing extremism.
In 2017, it is calculated that there were 950 attacks on Muslims and mosques in Germany alone. Many of last year’s attacks in America involved a common right wing extremist hatred of Islam, and a targeting of Muslims, joining a long-standing enmity towards Jews.
Almost all recent terrorist attacks have been lone-actor attacks. They are notoriously difficult to predict. Whether inspired by Salafi jihadi Islamist extremism or right wing extremism, lone-actor attacks commonly feature individuals fixated on the deluded dream of going from “zero to hero”.
One of the main reasons authorities struggle with identifying right wing extremist “nobodies” who post online, before they turn to violence, is that it’s difficult to pick up a clear signal in the noise of a national discourse increasingly dominated by exactly the same narrative elements of mistrust, anxiety, and a blaming of the other.
In Australia, as in Europe and America, mainstream politicians and mainstream media commentators have increasingly toyed with extremist ideas in the pursuit of popularity. Many have openly brandished outrageous ideas that in previous years would have been unsayable in mainstream political discourse or commentary.
Donald Trump can be deservedly singled out for making the unspeakable the new normal in mainstream right wing politics, but he is hardly alone in this. And sadly, for all of the relative civility and stability of Australian politics, we too have now come to normalise the toxic politics of fear.
No-one put it better than The Project host Waleed Aly in saying that Friday’s terrorist attacks, although profoundly disturbing, did not come as a shocking surprise. Anyone who has been paying attention and who really cares about the well-being and security of Australian society has observed the steady growth of right wing extremist and right supremacist ideas in general, and Islamophobia particular.
They have seen the numerous attacks on Muslims and Jews at prayer and worried about the day when the murderous violence that has plagued the northern hemisphere will visit the southern hemisphere. But more than that, they have worried about the singling-out of migrants, and in particular asylum seekers, African youth and Muslims as pawns to be played with in the cynical politics of fear.
Scott Morrison is right to say these problems have been with us for many years. But he would do better to point out that our downward trajectory sharply accelerated after John Howard’s “dark victory” of 2001. The unwinnable election was won on the back of the arrival of asylum seekers on the MV Tampa in August followed by the September 11 attacks, and at the price of John Howard and the Liberal party embracing the white supremacist extremist politics of Pauline Hanson.
Both major parties, it must be said, succumbed to the lure of giving focus groups and pollsters the tough language and inhumane policies the public appeared to demand and reward. We are now beginning to see the true price that we have paid with the demonising of those arriving by boat seeking asylum, or looking too dark-skinned, or appearing too religious.
The result has been such a cacophony of hateful rhetoric that it has been hard for those tasked with spotting the emergence of violent extremism to separate it from all the background noise of extremism.
There are, of course lessons to be learned. Authorities need to do better. We can begin with a national database of hate crimes, with standard definitions and robust data collection. Clearly, we need to pay attention to hateful extremism if we are to prevent violent extremism.
But ultimately, we need to address the permissive political environment that allows such hateful extremism to be promulgated so openly. The onus is on commentators and political leaders alike. They cannot change the past, but they will determine the future.
Greg Barton, Chair in Global Islamic Politics, Alfred Deakin Institute for Citizenship and Globalisation, Deakin University
Have you played Monopoly lately? Or maybe snakes and ladders? These board games are examples of 100-year-old games that many still play today.
But the way they are played today may not be teaching the lessons their designers hoped to share.
At the start of the 20th century, children were part of the regular workforce. They possessed few toys. When U.S. manufacturers created games, they built them to market to parents: to teach as well as to entertain.
Monopoly didn’t become a hit until the Depression. Its original message that all should benefit from wealth was transformed to its current version — where you crush opponents by accumulating wealth — by its second developer, an unemployed heating engineer named Charles Darrow. By the mid-1930s, orders for the game had become so extensive that employees of Parker Brothers stared piling the order forms in laundry baskets.
Gavitt’s Stock Exchange (1903), a precursor to the modern day card game Pit.
Strong Museum of Play, 109.11515
Games with meaning
Many of the games in circulation today are more than a century old. Pitt (originally Gavitt’s Stock Exchange) was made during economic panics, railroad failures, speculation and anti-monopoly movements. Patented by Harry E. Gavitt in 1903, the game was designed (as the rulebook says), to reproduce the “excitement and confusion generally witnessed in stock and grain” exchanges.
Players work to gain a monopoly over an economic market. They gather all the copies of one product and inflate its value to reap substantial profits.
Monopoly and Pitt taught economics while Chutes and Ladders focused on morality.
Chutes and Ladders was inspired by games played in South Asia about 1,000 years ago. Many of these games had explicit Hindu religious themes. They had different names: Nepal (Nāgapāśa); Tibet (The Game of Liberation); and India (Jñāna Chaupār). A Buddhist monk, Sa-skya Pandita, created the Game of Liberation for his sick mother in the 13th century. He likely based it on earlier forms of the game he encountered as part of his pilgrimages.
In Nāgapāśa, players attempted to reach a realm of one of the Hindu gods. In the Game of Liberation, they aimed to reach nirvana.
Toys and games offered a way for teachers and parents to prepare children for their adult lives. Parents used mechanical toys to teach engineering to boys. They used dolls to teach sewing, ingenuity, and household management to girls. It was one way to take complex ideas about society and translate them into forms children could understand.
Playing games could also be a way to learn history. During the the Philippine-American War, game designers created Merry War to teach children about the conflict.
Merry War: A Battle Game for Boys (1899) has U.S. and Filipino soldiers battle against one another.
By the 1960s, manufacturers began to advertise directly to children, rather than to their parents. They emphasized the excitement of their products over their educational value.
At the same time, civil rights unrest, the rise of feminism and rapid technological innovation made the world seem unpredictable. How could you prepare your children for their adult lives when the future seemed so difficult to understand?
Today, lessons remain embedded in many board games, but they sit apart from games just for fun. Board games are no longer a key venue to transmit information across generations.
Yet for all that has changed, we still play these old games, even if we don’t remember their lessons.
Everyone knows that you should not look at the sun!
Not with your naked eye, not with sunglasses and certainly not with binoculars or with a telescope. Our sun might be just an ordinary star, but it’s extremely close to us — about 269,000 times closer than the next nearest star. This makes the sun very, very bright.
Everyone knows that you should not look at the sun. But what about during an eclipse? This situation will confront us on Aug. 21, when the entirety of North America, along with parts of South America, Africa, Europe and eastern Russia, will experience a solar eclipse.
For the vast majority of viewers, including anyone in any part of Canada, the eclipse will be a partial one. This means that the moon will block out part of the face of the sun but leave the rest of it unchanged.
NASA’s Solar Dynamics Observatory saw a partial solar eclipse in space when it caught the moon passing in front of the sun on May 25, 2017.
If you’re under the path of the partial eclipse — even somewhere where the sun is 99 per cent concealed — you still should not look at the sun with the unaided eye. Even one-hundredth of the sun’s normal brightness is enough to permanently damage your eyesight.
For some lucky viewers in parts of 14 U.S. states, a total solar eclipse awaits on Aug. 21. This will be far more exciting than a mere partial eclipse. For maybe as long as two minutes, depending on your exact location, the sun will disappear completely behind the moon. The temperature will drop, the stars will come out, and the birds will think evening has come.
If you are under the path of the total eclipse, you’ll likely have more than an hour of partial eclipse both before and after the exciting moment of totality. During the partial phases, the usual rules apply: Wear your eclipse glasses or use your colander, but don’t look at the sun unaided!
However, when the time finally arrives and when the sky goes dark, it will finally be safe to look. Take off your glasses, stare at the sun with your unaided eyes, and soak up a remarkable cosmic moment.
The Hinode satellite observed the sun’s corona during a total solar eclipse on July 22, 2009.
During the total eclipse, it is completely safe to look at the sun without any equipment at all. And what a sight it will be.
Revealed, just for a moment, will be the sun’s glorious corona, the faint tendrils of ultra-hot gas that stream off the sun’s blazing surface. This is not to be missed. If you leave your eclipse glasses on, you won’t see anything.
After a minute or two, the total eclipse will be over, the skies will lighten and special safety precautions must once again be taken. But those who experience totality will be left with memories of an otherwise hidden view of the Universe, a brief glimpse of our life-giving sun unlike any other.
The mass shooting at the Tree of Life synagogue in Pittsburgh exemplifies an increasingly deadly form of domestic terrorism committed by far-right extremists: the targeting of institutions and individuals due to their religious affiliation.
Unfortunately, it’s not new for far-right extremists to vilify non-white, non-Anglo-Saxon and non-Protestant religions. Judaism has endured most of their ideological rage and conspiratorial paranoia. For more than a century, extreme far-right ideologues have peddled anti-Semitic and racist conspiracy theories. Their dogma claims, falsely, that globalist Jews have infiltrated the government and other U.S. institutions, and that Jews and non-whites pose an existential threat to the white race.
Some more militant members of the extreme far-right have acted on these beliefs by attacking Jewish people and institutions. The ultimate goal for many, according to the information we collect about perpetrator motives, is to ignite a race war in which Anglo-Saxon whites will emerge victorious – such that they can reclaim power over the U.S. political system and social institutions.
Patterns of religious animosity
Since 2006, the U.S. Extremist Crime Database has been a reliable source of information on extreme far-right homicides. We and other terrorism researchers have used this database to understand the nature of violent and non-violent extremist crimes in the U.S.
From 1990 to the present, far-right extremists have committed 217 ideologically motivated homicides. Of these homicides, 19 targeted religious institutions or individuals thought to be associated with a particular religion. Eleven were motivated by anti-Semitism, specifically.
More than three-quarters of these homicides had only one victim; however, many events had multiple fatalities. Due to this, the total number of ideological homicide victims was 490, including the 168 murdered in the Oklahoma City bombing. Of those victims, more than 50 were murdered because the offender targeted an institution or individual based on religious affiliation, real or perceived.
Although religious minorities are murdered less frequently than racial and other social minorities, an increasing number of lethal attacks by extreme far-rightists have drawn more attention to this form of violence.
In addition, there have been close to 100 failed or foiled plots against Jewish institutions or individuals between 1990 and 2014. These plots, some involving attempted murders, rarely receive the same amount of attention as successful murders. However, the fact that failed or foiled plots are an estimated nine times as prevalent as similarly motivated homicides during this time frame is cause for concern.
Moreover, ECDB data on anti-Semitic homicides point to a disturbing trend. Far-right extremists are engaging in deadlier attacks within the most sacred of spaces: houses of worship. There is no indication that extreme far-rightists will cease propagating anti-Semitic conspiracies. And it is also likely that some will interpret these twisted messages as permission to kill religious minorities. As in in the past, some may even perceive doing so as a higher calling or sacred duty.
The trauma stemming from these attacks will have severe and long-lasting psychological effects on the victims, their families and the broader Jewish community. In this way, crimes targeting religious minorities and other protected groups are unique from parallel crimes and rip deeper at America’s social fabric.
We, as a society, may not know what exactly pushes one person to act so violently on their beliefs and another to not. But we believe countering divisive narratives with different viewpoints informed by evidence on what works to prevent radicalization is more productive than aggravating wounds with politicized rhetoric.
As Americans, we must speak openly about the perils of white supremacy, anti-Semitism and both the rhetorical and real dehumanization of those we perceive as unlike us. Those wielding political power and influence need to publicly and clearly condemn acts of violence by extreme far-rightists and the ideologies underpinning this form of domestic terrorism.
Dr. Steve Chermak at Michigan State University and Dr. Joshua D. Freilich at John Jay College of Criminal Justice contributed to this research.
If a man offers to help a woman with her heavy suitcase or to parallel park her car, what should she make of the offer?
Is it an innocuous act of courtesy? Or is it a sexist insult to her strength and competence?
Social psychologists who describe this behavior as “benevolent sexism” firmly favor the latter view.
But researchers have also revealed a paradox: Women prefer men who behave in ways that could be described as benevolently sexist over those who don’t.
How could this be?
Some say that women simply fail to see the ways benevolent sexism undermines them because they’re misled by the flattering tone of this brand of kindness. Psychologists have even suggested that benevolent sexism is more harmful than overtly hostile sexism because it is insidious, acting like “a wolf in sheep’s clothing.”
As social psychologists, we had reservations about these conclusions. Aren’t women sophisticated enough to be able to tell when a man is being patronizing?
Surprisingly no previous research had tested whether women do, in fact, fail to recognize that benevolent sexism can be patronizing and undermining. And given our backgrounds in evolutionary theory, we also wondered if these behaviors were nonetheless attractive because they signaled a potential mate’s willingness to invest resources in a woman and her offspring.
So we conducted a series of studies to further explore women’s attraction to benevolently sexist men.
What does benevolent sexism really signal?
The concept of benevolent sexism was first developed in 1996. The idea’s creators argued that sexism is not always openly hostile. To them, attitudes like “women should be cherished and protected by men” or behaviors like opening car doors for women cast them as less competent and always in need of help. In this way, they argued, benevolent sexism subtly undermines gender equality.
Since then, social psychologists have been busy documenting the pernicious effects that benevolent sexism has on women.
Whereas men can successfully reproduce by providing a few sex cells, a woman’s reproductive success must be tied to her ability to complete months of gestation and lactation.
During much of human history, a woman’s ability to choose a mate who was able and willing to assist in this process – by providing food or protection from aggressors – would have increased her reproductive success.
Evolution, therefore, shaped female psychology to attend to – and prefer – mates whose characteristics and behaviors reveal the willingness to invest. A prospective mate’s muscular physique (and, today, his big wallet) certainly indicate that he possesses this ability. But opening a car door or offering his coat are signs that he may have the desired disposition.
Women weigh in
In our recently published research, we asked over 700 women, ages ranging from 18 to 73, in five experiments, to read profiles of men who either expressed attitudes or engaged in behaviors that could be described as benevolently sexist, like giving a coat or offering to help with carrying heavy boxes.
We then had the participants rate the man’s attractiveness, willingness to protect, provide and commit, and their likelihood of being patronizing.
Our findings confirmed that women do perceive benevolently sexist men to be more patronizing and more likely to undermine their partners.
But we also found that the women in our studies perceived these men as more attractive, despite the potential pitfalls.
So what made them more attractive to our participants? In their responses, the women in our study rated them as more likely to protect, provide and commit.
We then wondered whether these findings could only really be applied to women who are simply OK with old-fashioned gender roles.
To exclude this possibility, we studied participants’ degree of feminism with a widely used survey that measures feminist attitudes. We had them indicate their level of agreement with statements such as “a woman should not let bearing and rearing children stand in the way of a career if she wants it.”
We found that strong feminists rated men as more patronizing and undermining than traditional women did. But like the other women, they still found these men more attractive; the drawbacks were outweighed by the men’s willingness to invest. It seems that even staunch feminists may prefer a chivalrous mate who picks up the check on a first date or walks closer to the curb on a sidewalk.
In this time of fraught gender relations, our findings may provide reassurance for women who are confused about how to feel towards a man who acts chivalrous, and well-meaning men who wonder whether they should change their behavior towards women.
But several interesting questions remain. Does benevolent sexism always undermine women? It might depend on context. A male being overly helpful to a female co-worker in a patronizing way might hurt her ability to project professional competence. On the other hand, it’s tough to see the harm in helping a woman move heavy furniture in the home.
Understanding these nuances may allow us to reduce the negative effects of benevolent sexism without requiring women to reject the actual good things that can arise from this behavior.
An estimated 400,000 Americans are currently living with multiple sclerosis, an autoimmune disease where the body’s immune cells attack a fatty substance called myelin in the nerves. Common symptoms are gait and balance disorders, cognitive dysfunction, fatigue, pain and muscle spasticity.
Colorado has the highest proportion of people living with MS in the United States. It is estimated that one in 550 people living in the state has MS, compared to one in 750 nationally. The reason for this is unknown, but could be related to several factors, such as vitamin D deficiency or environment.
Currently available therapies do not sufficiently relieve MS symptoms. As a result many people with the condition are trying alternative therapies, like cannabis. Based on several studies, the American Association of Neurology states that there is strong evidence that cannabis is effective for treatment of pain and spasticity.
Although there are many anecdotal reports indicating cannabis’ beneficial effects for treatment of MS symptoms such as fatigue, muscle weakness, anxiety and sleep deprivation, they have not been scientifically verified. This is because clinical trials – where patients are given cannabis – are difficult to do because of how the substance is regulated at the federal level.
To learn more, my Integrative Neurophysiology Laboratory at Colorado State University is studying people with MS in the state who are already using medical cannabis as a treatment to investigate what MS symptoms the drug can effectively treat.
An MRI scan of a fixed cerebral hemisphere from a person with multiple sclerosis.NIH Image Gallery/Flickr, CC BY-NC
Medical marijuana isn’t a prescription drug
Marijuana, or cannabis, contains over 100 compounds, but THC (Tetrahydrocannabinol) and CBD (Cannabidiol) are believed to have the most medical relevance.
However, there is currently no information about the most effective ratio of THC and CBD, which form of ingestion (smoking or eating, for instance) is best, or how often people with MS should use cannabis products.
The main reason for the limited scientific evidence about how well cannabis can treat MS symptoms is because it is a Schedule 1 substance. This means that it has “no currently accepted medical use and a high potential for abuse.” This classification makes it very difficult to study cannabis in clinical trials.
Because cannabis is on Schedule 1, doctors can’t prescribe it, even in the states with medical marijuana laws, like Colorado. In those states doctors can provide patients with a “permission slip” for cannabis, which has to be approved by a state agency.
Because of the lack of scientific evidence, doctors can’t recommend a specific strain and dosage of cannabis to patients. Patients are left to choose on their own. Moreover, a recent study in the Journal of the American Medical Association showed that out of 75 cannabis products, only 17 percent were accurately labeled. And 23 percent contained significantly more THC than labeled, possibly placing patients at risk of experiencing adverse effects.
David Sloan, a multiple sclerosis patient and author of the memoir ‘One day at a Time,’ exhales smoke from medical cannabis concentrate.AP Photo/Brennan Linsley
How we are studying cannabis and MS
My lab’s long-term goal is to determine whether cannabis can safely and effectively treat MS symptoms. But because of current federal regulations our lab can conduct only observational studies at this time. To conduct clinical trials with a Schedule 1 substance, investigators must have a special license, which my lab is in the process of applying for. At the moment, this means we study only people who are or are about to use cannabis and we do not provide cannabis to anyone for our studies.
We recently completed an online survey of 139 MS patients currently using cannabis to learn what types of products they used, how often they used those products and for how long.
Our results, which have not yet been published, found that 91 of our respondents (66 percent) reported that they currently use cannabis, and 56 percent of the cannabis users reported using either smoked or edible products. Seventy-eight percent of the cannabis users also indicated that they reduced or even stopped other medications as a result of their cannabis use.
The survey respondents who are using cannabis reported lower disability scores on the Guy’s Neurological Disability Scale, a clinical scale used to evaluate neurological disability in people with MS, and they seem less likely to be obese. However, these data are self-reported, which means objective longer clinical trials are required to confirm these results.
We are also conducting an ongoing observational study, set to be completed in mid-2017, on the effects of regular cannabis use on physical function and activity levels in people with MS. There are many studies on the influence of cannabis on cognitive function in healthy and diseased populations. However, no study to date has used objective measures of motor function in people with MS who are using cannabis, such as muscle strength and fatigue tasks, walking performance and postural stability tests.
Our preliminary results indicate that people with MS using cannabis have greater physical activity levels, leg strength and walking speed, while also having less spasticity, fatigue and a lower perceived risk of falling. It is of note that these individuals are rarely using only cannabis to help control their symptoms. They are often using cannabis alongside traditional medications.
Importantly, cannabis users did not perform worse than nonusers on any of our measurements. These are very promising results, and we are expecting significant positive effects of cannabis at the end of this observational study.
Randomized control trials are needed
The outcomes of these observational studies will be the foundation for larger randomized clinical trials, where some patients are treated with cannabis and others aren’t. These types are studies are needed to truly show the benefits and risks of consequences of cannabis use in this population.
Applying for the special license that investigators must have to conduct clinical research with a Schedule 1 substance is a lengthy process. Once granted, the DEA requires on-site inspections of the investigator’s facilities. Furthermore, it is also very difficult for these types of experiments to be approved and performed. These policies make conducting research on the medical benefits and side effects of cannabis in the United States extremely hard. As a sad result, top researchers are looking to export their ideas outside the country.
We want to conduct clinical research to understand what cannabis products MS patients should use, in what dosage and in what form of ingestion. We also want to find out whether long-term cannabis use is safe, and if the effectiveness changes over time due to increased tolerance. Fortunately, our first intervention study, which will investigate the effects of different marijuana strains on motor and cognitive function in people with MS, has been approved by the CSU Institutional Review Board. This means that my lab can begin this research once our license is approved.
The answers to these questions will provide guidelines for health care providers and people with MS on cannabis use. If these studies can demonstrate that cannabis effectively relieves and treats MS symptoms, they could help establish the medicinal value of cannabis. That could make a case for rescheduling cannabis, making it easier for physicians and researchers to establish cannabis’ true benefits and risks.
Many legitimate questions arise whenever tragic events happen. When high-profile persons are affected, the conversation becomes a national one. With news of the growing increase in nonpharmaceutical versions of fentanyl coming in from China and Mexico, the conversation broadens to an international one. How can we prevent deaths from overdose of this potent drug?
Let’s address some of the most frequently asked questions I’ve heard about fentanyl recently, but before we do that, I want to put you in my shoes for a minute.
I am an anesthesiologist. To an anesthesiologist, fentanyl is as familiar as a Philips screwdriver is to a carpenter; it is an indispensable tool in my toolbox. It is the most commonly used painkiller during surgery. If you’ve had surgery, it is more likely than not that you have had fentanyl. Fentanyl is used to blunt airway reflexes and to place the breathing tube into the trachea with minimal coughing. It is the potent analgesic that prevents pain from the surgeon’s scalpel while your body sleeps under anesthesia. It is also the painkiller that allows you to wake from anesthesia without feeling existential pain in the immediate recovery room once the gases are turned off. Fentanyl is used to enable millions of people to undergo major surgery in the United States every day.
Before fentanyl existed, there were morphine and other similar, relatively weak opioids that were insufficient for the type of major surgery that happens today. To treat major surgical pain, morphine is not only too weak but it is slow and, once given, lasts a long time. And since opioids slow and stop your breathing, historically, patients who received large doses of morphine for surgery had to remain in intensive care units with the breathing tube in place for a long time after surgery until the morphine wore off. And doubly adverse, morphine causes histamine release in the body, resulting in cardiovascular side effects like low blood pressure – not a good thing to have during surgery if you want to wake up with working organs.
The precision and timing of modern surgery required a painkiller that was fast-acting, potent enough to blunt pain from a scalpel, stable enough not to cause cardiovascular problems, and short-acting enough to enable removal of the breathing tube once the surgery was over.
Fentanyl was developed by Dr. Paul Janssen in Belgium during the 1960s to meet precisely this need, and it contributed to the expansion and safety of surgery we do today. In fact, the expansion of open-heart and bypass surgery in the 1970s depended on concurrent progress in the safety of anesthesia through the use of fentanyl.
In the hands of an anesthesiologist who is licensed to prescribe and dispense fentanyl in the operating room, the drug is safe, even given its potency. Unmonitored, it can easily lead to death, as it essentially causes a person to stop breathing.
You may wonder: Isn’t there something safer?
Yes, there are alternatives, but they are not necessarily safer. There are other, even more potent opioids like sufentanil and shorter-acting opioids like alfentanil and remifentanil, most of which are much more expensive but not any safer. There are non-opioids such as ketamine, lidocaine and ketorolac that are used for surgical pain, and these are being utilized more and more to spare the need for large doses of opioids. There are even ways to do surgery under regional anesthesia, where the anesthesiologist can make the region of your body numb and unable to feel anything or very little so that opioids are not required.
But you can’t take your anesthesiologist home, and sometimes a person experiences severe, persistent, pain post-surgery.
Why would anyone need to take fentanyl at home? There are a few reasons, but the most common reason is tolerance. People with prolonged, severe pain who continue to use opioids will experience tolerance as their bodies becomes used to the pain medicine over time. To continue to treat the persistent pain, they may need a dose increase. Eventually some patients end up on very potent opioids like fentanyl.
Persistent pain can occur from surgery, trauma or chronic illness. Cancer is a big one. It can be a source of unending, intense pain, and we treat that with the best tools we have. Over time, as patients become tolerant to weaker opioids, the more potent opioids are needed to control the pain. Fentanyl is one of those drugs strong enough to treat major surgical and unending cancer pain that has become tolerant to other opioids.
Good drug, killer drug
So this begs the question: What happens when a person who is not opioid-tolerant takes fentanyl?
Anesthesiologists give fentanyl and are expert at controlling a patient’s airway and keeping them breathing while they are being observed. Pain physicians prescribe fentanyl in a very controlled manner and only after a patient has been observed and deemed tolerant to weaker opioids.
So, when someone who is not tolerant to opioids takes fentanyl, it is very easy to overdose, to stop breathing and to never wake up. It is very easy for those who do not use these potent painkillers as prescribed to overdose.
Fentanyl can be used safely if used as prescribed, but it is a killer on the streets. Fentanyl analogues are relatively easy to synthesize and are often mixed with heroin or benzodiazepines to quicken the onset and enhance the high. A simple Reddit search reveals the many forms of fentanyl that are being synthesized and sold illegally and the countries it is being smuggled in from. Even the users and dealers there warn about its potential for easy overdose. Indeed, many users don’t even know the heroin or xanax they have bought on the street is laced with fentanyl until it is too late.
Do we need fentanyl, and have we contributed to its abuse? This is a question we ask ourselves as we struggle to get a grip on the modern opioid epidemic, tragedies like the death of Prince and patients who suffer from pain and addiction.
Can we do without medications like fentanyl altogether? Right now, we cannot do without opioids entirely. We would need potent alternatives with limited side effects. The alternative tools we have are insufficient to enable us to quit opioids cold turkey.
A sort-of transition plan has developed in the medical community where we use multiple non-opioid pain medications in combination with nonmedication treatments, such as mindfulness, behavioral therapy and education to minimize the need for opioids. In many instances, these creative efforts have enabled opioid-free options for specific major surgeries. The good news is that the demand for change has reached the top levels of government, hospitals and patient organizations. Money for research and education is being made available. New laws are being enacted. A revolution in pain management is necessary and, hopefully, imminent.
A recent study by the National Institutes of Health found that more than one in three people in the United States have experienced pain of some sort in the previous three months. Of these, approximately 50 million suffer from chronic or severe pain.
But unlike treatments for diabetes, cancer and heart disease, therapies for pain have not really improved for hundreds of years. Our main therapies are non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or aspirin, which are just modern versions of chewing on willow bark; and opioids, which are derivatives of opium.
In 2012 259 million prescriptions for opioids were filled in the United States. It is not clear how many of these prescriptions were for chronic pain. And indeed, new CDC guidelines on the use of opioids to treat noncancer chronic pain caution physicians to consider the risks and benefits of using opioids when prescribing them to patients.
The fact is, however, that opioids are used to treat chronic pain not because they are the ideal treatment, but because for some patients, despite their drawbacks, they are the most effective treatment available at the moment.
The problem, as I see it, is this: we are not investing enough in researching and teaching what causes pain and how to treat it.
Pain Can Have a Purpose
I study the processes that trigger and maintain chronic pain. One of the first things I teach my students is that pain is a biological process that is critical for life. Pain protects our bodies from injury and by reminding us that tissue is damaged and needs to be protected it also aids in repairing the injuries we do acquire.
This is graphically illustrated by individuals who are congenitally incapable of feeling pain. People with these conditions typically succumb to infections or organ failure at a young age due to multiple injuries that go unattended. Because they cannot feel pain, they never learn to avoid hazards, or how to protect still-healing injuries.
For the most part, physicians and scientists are not particularly concerned with pain from everyday bumps, bruises and cuts. This type of acute pain typically does not require treatment or can be treated with over-the-counter medication. It will resolve itself when the tissue heals.
What concerns those of us who treat and study pain, however, is chronic pain. This type of pain—that can last for weeks, months or even years—serves no useful purpose for survival and is actually detrimental to our health.
There isn’t one type of chronic pain.
In many cases chronic pain persists after an injury has healed. This happens relatively often with wounded veterans, car accident victims and others who have suffered violent trauma.
Chronic pain from arthritis is telling the person about the damage in their body. In this respect it is similar to acute pain and, presumably, if the body healed the pain would subside. But, at the moment, there is no treatment or intervention to induce that healing so the pain becomes the most troubling aspect of the disease.
Chronic pain can also arise from conditions, like fibromyalgia, which have an unknown cause. These conditions are often misdiagnosed and the pain they produce may be dismissed by health care professionals as psychological or as drug-seeking behavior.
The human pain experience can be divided into three dimensions: what pain researchers call the sensory-discriminative, the affective-motivational and the cognitive-evaluative. In acute pain there is a balance between each of these dimensions that allows us to accurately evaluate the pain and the threat it may pose to our survival. In chronic pain these dimensions are disrupted.
The sensory-discriminative dimension refers to the actual detection, location and intensity of the pain. This dimension is the result of a direct nerve pathway from the body to the spinal cord and up into the brain’s cortex. This is how we are aware of the location on our bodies of a potential injury and how much damage may be associated with the injury.
Knowing where it hurts is only part of experiencing pain. Is your injury life-threatening? Do you need to run away or fight back? This is where the affective-emotional dimension comes in. It arises from the pain circuitry interacting with the limbic system (the emotional centers of the brain). This adds an emotional flavor to the incoming pain signal and is part of the fight-or-flight response. This pathway evokes the anger or fear associated with the possibility of physical harm. It also provokes learning so that in the future we avoid the circumstances leading to the injury.
The third dimension, the cognitive-evaluative, is the conscious interpretation of the pain signal, combined with other sensory information. This dimension draws on the different aspects of pain processing allowing us to determine the location and potential severity of an injury and to come up with survival strategies based on all available information.
The pain sensory system is designed for survival. If a pain signal persists, the default programming is that the threat to survival remains an urgent concern. Thus, the goal of the pain system is to get you out of harm’s way by ramping up the intensity and unpleasantness of the pain signal.
To increase the urgency of the pain signal, the sensory-discriminative dimension of pain becomes less distinct, leading to a more diffuse, less localized, pain. This pathway also amplifies the pain signal by rewiring spinal cord circuits that carry the signal to the brain, making the pain feel more intense.
If there is a threat to survival, the increasing intensity and unpleasantness of pain serves a purpose. But if the pain signal persists from, let’s say, arthritis or an old injury, the increased intensity and unpleasantness is unwarranted. This is what we define as chronic pain.
In chronic pain, as compared to acute pain, the affective-motivational dimension becomes dominant, leading to psychological consequences. Thus suffering and depression are much worse for chronic pain patients than it would be for an individual with an equivalent acute injury.
The multifaceted nature of pain is why opioids are often the most effective agents for both moderate to severe acute and chronic pain.
Opioids act at all levels of the pain neural circuitry. They suppress incoming pain signals from the peripheral nerves in the body, but importantly for chronic pain patients, they also inhibit the amplification of the signals in the spinal cord and improve the emotional state of the patient.
Unfortunately, patients rapidly develop tolerance to opioids, which significantly reduces their effectiveness for chronic therapy. Because of this as well as their addictive nature, potential for abuse and overdose, and side effects such as constipation, opioids are less than ideal agents for treating chronic pain. It is critical that we find alternatives. But that’s easier said than done.
Funding for Pain Research Lags
In 2015 the National Institutes of Health spent US$854 million on pain research, compared to more than $6 billion for cancer. It is no wonder that pain patients muddle through with what amounts to centuries-old therapies.
The competition for funding for pain researchers is intense. In fact, many of my friends and colleagues, all highly experienced midcareer scientists, are leaving research because they cannot sustain the funding necessary to make any significant progress in finding treatments for pain. I, myself, spend up to 30 hours per week preparing and writing research proposals for funding agencies. Yet, less than one in 10 of these proposals are funded. The dearth of funding is also discouraging young scientists from doing pain research. With tenure at major universities becoming more and more difficult to attain, they can little afford to spend all of their time writing research proposals that do not get funded.
In addition, many medical and dental programs in the United States devote as little as one hour in their curriculum to teaching pain mechanisms and pain management. Thus, most of our health professionals are poorly prepared to diagnose and treat chronic pain, which contributes to both the under treatment of pain and the abuse of opioids.
Unrelieved pain contributes more to human suffering than any other disease. It is time to invest in research to find safe effective therapies and on training health care providers to appropriately diagnose and treat pain.
Budweiser, the so-called King of Beers, may be on its last kegs.
It may seem odd to picture the demise of the flagship brand of the world’s largest beer company. But Anheuser-Busch – the U.S.-based unit of AB InBev – is following in the footsteps that led to the irrelevance of a host of other once-dominant companies – Eastman Kodak, Woolworth’s Department Stores, Bethlehem Steel and Blockbuster Video, to name a few.
While AB InBev shareholders are cheering each move to boost short-term profitability by snapping up other companies – including the US$110 billion takeover of rival SABMiller – CEO Carlos Brito may be unwittingly digging Anheuser-Busch’s grave by ignoring long-term trends.
How could the rational pursuit of profits and growth through acquisition mean the beginning of the end for Anheuser-Busch?
This, we would argue, is a case of disruption theory in action. And the disruptors are the growing ranks of craft brewers that are collectively changing the industry and beer consumption habits as consumers increasingly shun Anheuser-Busch and its products – the disrupted – for beers made locally and with a wider variety of higher-quality ingredients.
It’s something we’ve witnessed firsthand, in our own research and through an online community called Crafting A Strategy that two of us set up to share knowledge in the beer industry.
New market disruption
Harvard Business School Professor Clay Christensen coined the phrase “disruptive innovation” in 1995 to describe how a new product or service initially takes root at the bottom of a market and then relentlessly moves upmarket, eventually displacing established competitors.
You could make Coors from swamp water and it would be exactly the same.
The repeal of Prohibition in 1933 didn’t include home brewing, which meant few people knew how to brew and new brewery start-ups were rare. The number of brewers dwindled from several thousand prior to Prohibition to about 100 in the late ‘70’s.
That marked a turning point, as a new federal law finally made home brewing legal again. But other laws remained in force in the ‘80’s and '90’s that didn’t allow early craft brewers to sell directly to consumers, forcing them to first sell to a wholesaler that would then distribute the beer to a retail grocer or bar. This system meant the only way to make a reasonable profit was to go big and leverage economies of scale to ensure your product was featured by distributors.
Revelers celebrate with a pint after prohibition is repealed.Bar drinking via www.shutterstock.com
2. Customers who use the product need to go to an inconvenient, centralized location.
There were only 89 breweries in America in the late 1970s, and their distribution model meant that consumers had very few choices. In particular, they had inconvenient or no access to craft beer. They generally drank Bud, Pabst, Schlitz, Miller, Coors, etc. By 1981, these brewers controlled 76 percent of the U.S. market.
In other words, you had a large population without easy access to well-crafted beer and a system that centralized production and tightly controlled distribution. This created an opportunity for disruption, in the view of Christensen. The question was, would something change that allowed a larger population to make beer and sell the product more directly to consumers?
3. A technology/business model is developed so that a large population can begin owning and using, in a more convenient context, something that historically was available only in a centralized, inconvenient location.
In the beer story, that game-changing innovation was the brewpub business model. This became possible after laws began to change in the 1980s to allow over-the-counter sales of beer produced in-house.
Yakima Brewing and Malting Inc. opened in Washington state in 1982 and was closely followed by California’s Mendocino Brewing in 1983. The advent of microbreweries coincided with other industry trends that made it easier to make a profit from small production. There was also growing ideological opposition to the incumbent sector.
Collectively, these changes drove the craft beer revolution in the U.S.
Noted beer historian Dr. Martin Stack summed up the innovation this way:
Microbreweries represented a new strategy in the brewing industry: rather than competing on the basis of price or advertising, they attempted to compete on the basis of inherent product characteristics.
Disruption works because the initial business models or technologies of the eventual disruptors don’t perform as well as existing ones, so little attention is paid by the incumbents. N. Taylor Thompson succinctly summarized new market disruption as:
a cheaper, more accessible, and worse-performing (business model) that turns non-consumers into customers.
From a financial perspective, chasing a smaller group of nonconsumers (like craft beer drinkers) who want only beer that costs a lot to make seems like a relatively foolish use of assets. Instead, executives at AB InBev, which is also known for beers including Corona, Stella Artois and Michelob, understood that making light lagers at a 30 percent to 33 percent operating margin allowed them to earn the most money out of each dollar spent. They ignored craft for so long because craft breweries typically operate on an unattractive 2-5 percent margin.
While being ignored, craft beer producers learned and improved without needing to focus attention on direct competition from the large incumbents, pushing operating margins higher and getting the attention of wholesalers who were keen to the changing buying habits among beer drinkers. As a result, their operating margins soared, even as their scale remained relatively small. Boston Beer Company’s operating margins, for example, have crept up to 16.3 percent.
Brewers AssociationThe number of craft breweries has soared in recent years.Brendan McDermid/Reuters
The numbers say it all: while overall beer sales fell 0.2 percent in 2015, sales of craft surged 12.8 percent. Bigger craft brewers are building factories all over the U.S., and pipelines of expertise are flowing toward craft as Anheuser-Busch executives migrate over.
But AB InBev’s response continues to follow the “disrupted” playbook and typical strategy for mature companies: mergers and acquisitions to defend their existing space and to increase average margins through economies of scale.
Most recently, the company agreed to buy fellow behemoth SABMiller, maker of dozens of beers including Leinenkugel’s, Miller Lite and Peroni and another brewer chasing the same high-margin beers American consumers increasingly shun. Even attempts by SABMiller’s American division, MillerCoors, to create “crafty” beers are increasingly dismissed by consumers.
Here’s the irony: this merger equates to chasing a 30-33 percent margin on a $2 product (about $0.62) instead of investing in craft processes to make a 16-20 percent margin on a $5 product (about $0.90) that more and more people seem to want.
To make things worse for AB InBev, this craft beer movement seems to be not only spreading all over the U.S. but also the world.
AB InBev CEO Brito pours a Stella Artois beer after the annual shareholders meeting in Brussels in April.Francois Lenoir/Reuters
Cigar City likely left tens (perhaps hundreds) of millions of dollars on the table when it walked away from AB InBev. Late last year, for example, wine giant Constellation Brands paid $1 billion for the slightly larger craft brewer Ballast Point from California.
I was almost at the altar with someone else, but it never felt 100 percent right… It was a potentially life-changing opportunity and ultimately, I thought that I wasn’t going to be happy. No amount of money was going to make me happy.
And his customers, the ones helping drive the trends reshaping the beer industry, must be very pleased, because AB InBev’s strategies are creating a backlash. The fear is that by buying up craft breweries they’ll end up destroying what they represent.
Was Cigar City’s move foolish or wise? Redner opted for less money, a better corporate fit and greater control in brewing the product Cigar City’s customers expect.
Regardless of whether that strategy is successful, we believe this move signals a tectonic shift in the global beer industry. Specifically, craft beer has diminished big beer’s longstanding competitive advantages built on scale, distribution and laws that minimized competition from small-scale brewers.
Chasing higher profitability through lower-quality products and acquisitions might please shareholders, but it also fits nicely into disruption theory’s playbook where new technologies, laws, consumer awareness and business models actively work against the long-held advantages of incumbents.
In 20 years, will cracking open a Budweiser on a summer day still be commonplace? Or will it be a relic of times past? If AB InBev stays on its current strategic course, the latter, while tough to imagine now, is the more plausible scenario.
There are two opioid crises in the world today. One is the epidemic of abuse and misuse, present in many countries but rising at an alarming rate in the United States. The other crisis is older and affects many more people around the world each year: too few opioids.
Hospitals in the U.S.. and Europe routinely prescribe opioids for chronic cancer pain, end-of-life palliative care and some forms of acute pain, like bone fractures, sickle cell crises and burns. But patients with these conditions in much of Asia, Africa and Latin America often receive painkillers no stronger than acetaminophen.
Many factors play into this crisis, but I would argue that the International Narcotics Control Board (INCB), an independent monitoring agency established by the U.N.., is a fundamental cause of untreated pain in Asia, Africa and Latin America.
A worker handles medicine in the Pharmacie de la Sante Publique warehouse in Abidjan, Ivory Coast. Opioid painkillers can be difficult to access in many parts of Africa.Thierry Gouegnon/Reuters
Just how vast is the gap in pain relief?
In 2009, the U.S.., Canada and Europe accounted for 18 percent of global population, but 90 percent of global morphine consumption.
The global gap in access to opioids has been growing for a long time. In the U.S.., consumption of morphine in 2013 was 32 times higher than in 1964 (increasing from 2.3 mg per person to 79.9 mg per person). In the same time period, morphine consumption Tanzania only doubled to 0.15 mg person. In India in 2013, this figure was only 0.11 mg per person.
Per capita medicinal opioid consumption in Asia, Central America, the Caribbean and Africa is far below the INCB’s own minimum global standard. In countries and regions below this benchmark (set at 200 daily doses per million inhabitants per day), we can be certain that patients who need opioids for legitimate medical reasons do not receive them.
The INCB argues that poor countries have too few opioids because they cannot afford them. While there is a correlation between national income and national consumption of opioids, cost isn’t the principal issue.
Generic opioids are cheap. A generic 10mg immediate-release morphine sulfate tablet costs roughly US$0.01 to produce.
The main problem, I would argue, is a policy based on the fear that increased use of opioids will inevitably lead to abuse and trafficking. Palliative care physician and ethicist Eric Krakauer calls this fear “opiophobia.”
The work of the INCB has been crucial in increasing this fear of opioids and promoting restrictive policies that continue to keep millions of patients in unnecessary pain.
Morphine has legitimate medical uses.Vaprotan, via Wikimedia Commons, CC BY-SA
Fear of abuse drives ‘opiophobic’ policies
The International Narcotics Control Board has two purposes: to prevent addiction and to ensure the availability of opioids for legitimate medical use. But since its founding in 1968, the INCB has focused almost entirely on combating drug abuse, while ignoring access to pain relief.
One way the INCB tried to prevent addiction was by writing so-called “model laws” that it encouraged countries to enact. One such law, written in 1969, set controls on opioid prescription and distribution that were manageable for wealthier countries, but that would prove onerous in poor countries, particularly those with few doctors.
The Model Law stated, for instance, that opioids could be supplied only by doctors. This provision did not affect access to opioids in the United States or in other other wealthy nations with many physicians. But many poorer countries, where doctors were scarce, relied on nurses and other kinds of practitioners to prescribe drugs. The model law made no allowance for this.
In addition, the Model Law stated that physicians who prescribed opioids inappropriately or who failed to keep full records should be subject to “the same prison sentences and fines as are inflicted under the Penal Code for housebreaking.”
INCB laws were promoted by the United Nations Fund for Drug Control and Abuse (UNFDAC), which was founded in 1970. The UNFDAC conducted training sessions for national drug-control administrators and law enforcement to stress the dangers of abuse. But, as I found in my research, the sessions rarely mentioned the importance of access to pain relief.
The model laws and training sessions helped inspire countries in Latin America, Asia and Africa to pass new, more restrictive laws during the 1970s and ‘80s.
For instance, in India, a 1985 law required hospitals to obtain so many licenses before each shipment of morphine that many stopped using the drug at all. Medicinal morphine consumption in India fell by 97 percent between 1985 and 1997.
In Panama, nurses were barred from prescribing opioids. Paraguay and Guinea-Bissau mandated long prison sentences for any doctor who could not produce documentation justifying every single pill prescribed over years of practice. Fearing these punishments, doctors avoided prescribing opioids, even when they were medically necessary.
Cancer patients receive chemotherapy at Korle Bu Teaching Hospital in Accra, Ghana. Terminal cancer patients in Africa often cannot access opioid painkillers.Olivier Asselin/Reuters
Countries underestimate opioid needs in response to INCB pressure
The INCB also tried to prevent opioids prescribed to treat pain from being diverted into illegal markets by requiring every country to provide annual estimates of projected opioid needs for medical and scientific purposes. The INCB was responsible for approving these annual estimates, and tried to ensure that countries imported no more than the approved quantities.
Between the 1960s and the 1980s, INCB reports chastised many nations in Africa, Asia and Latin America for making estimates that it considered too high.
A country that imported more opioids than the INCB had approved risked a costly stain on its international reputation. The INCB could even recommend that countries impose trade embargoes on nations that produced or imported more opioids than it had deemed necessary. As a result, countries low-balled their estimates of future medicinal opioid requirements.
But the INCB didn’t judge these estimates based on actual medical need. Rather, it insisted estimates should be based on the number of physicians in a country, a potentially misleading piece of data in parts of the world were doctors are in short supply, and nurses and other health care professionals fill the gaps and prescribe medicine.
The INCB worried that too many opioid prescriptions could lead to abuse. Indeed, this is a major cause of the current addiction crisis in the United States. But, in the countries where the INCB exerted the greatest influence, the bigger problem was that too few (rather than too many) opioids were being prescribed.
A 1989 report from the INCB and World Health Organization revealed that national estimates of future opioid need were often calculated based on nothing more than previous years’ imports. That report also quantified the extent of untreated cancer pain, estimating that “at least 3.5 million cancer patients” worldwide “suffer needlessly from pain.”
The INCB is starting to change, slowly
For many years, the only thing most countries heard from the INCB was that their estimates were too high. But in 1999, the INCB announced it would begin to contact governments that submitted “particularly low estimates” to encourage them to increase their imports.
And in 2010, the INCB agreed that countries with few doctors should allow nurses to prescribe morphine, a reversal from previous policy recommendations.
But these small steps have not been enough to overcome the fear of opioids spread by decades of model laws and training sessions. The INCB’s recommendations continue to focus almost entirely on abuse.
For instance, a 2012 INCB report stated that national requests to import opioids sufficient to address existing need might be denied if such imports might raise “the possibility of diversion or abuse.”
More recent estimates from the World Health Organization suggest that each year 5.5 million terminal cancer patients and 1 million end-stage HIV/AIDS patients around the globe don’t get enough treatment, or any treatment at all, for their moderate to severe pain. The WHO estimates that tens of millions of people are denied medically necessary pain treatment every year.
Pain is universal, but its relief is still a function of geography.
For over a year, I’ve been documenting the lives of three long-term drug users – Marie, Cheryl and Johnny – who are participating in Vancouver’s heroin-assisted clinical study and program.
In recent years, heroin use in North America has exploded into an “epidemic.” At the same time, policymakers and the public have clashed over how to properly treat this public health scourge. Many heroin users receive methadone and other forms of treatment. However, some of the most vulnerable addicts haven’t responded to medication and detox.
I spent weeks building a rapport and trust with Marie, Cheryl and Johnny, who’ve all been addicted to heroin for years. They’ve each repeatedly tried detox and methadone and have been unable to stop using heroin.
In a sense, heroin-assisted treatment, a science-based, compassionate approach, is their last resort.
Those involved in the program – often users who haven’t sufficiently responded to other forms of treatment – receive pharmacological heroin in a clinical setting. While these programs have long been recognized as scientifically sound and cost-saving in countries like Switzerland, the Netherlands and Denmark, heroin-assisted treatment is only beginning to be offered in North America.
At first, the three subjects allowed me to take photos of them self-injecting their medication at Providence Health Care’s Crosstown Clinic in Vancouver’s Downtown Eastside. Slowly, over a period of weeks and months, they let me document their lives outside the clinic.
While I hoped to inform the public about heroin-assisted treatment, I also wanted to see if I could create visual counter-narratives to challenge the dominant tropes of drug genre photography.
More than anything, I wanted to represent Marie, Cheryl and Johnny as human beings – and show that their drug use didn’t define who they were, even though that’s how heroin users are usually depicted by documentary and news photographers.
The best way to do this, I realized, was to show them the photographs I’d selected and give them the opportunity to respond. I included their words with each photograph in the series.
‘Dark, seedy, secret worlds’
Before beginning my project, I had explored the work of some of the most influential drug genre photographers, and found that most of them have consistently represented heroin users as exotic, primitive and dangerous to society.
“There is a tendency in drug photography to attempt to make images of dark, seedy, secret worlds,” writes criminologist John Fitzgerald.
This can have the effect of “othering” the subjects – the idea that after looking at these kinds of images, viewers might look at drug users as outcasts.
Larry Clark’s 1971 photo work “Tulsa” is considered an exemplar of documentary photography. Many view the series, which depicts teenagers experimenting with drugs, sexuality and guns, as brutally honest and revealing.
In this photograph from his seminal work ‘Tulsa,’ photographer Larry Clark eroticizes the risky behavior of teens.Larry Clark, 'Couple,' Tulsa, 1971.
Clark’s follow-up photo essay, “Teenage Lust,” published in 1983, also focused on drug users in a voyeuristic, unsettling and erotic way.
The problem with this approach is that it creates sensationalized images, which, in turn, influence the public’s thinking and policymakers' decisions about how to treat drug users.
“For Clark the drug user is a modern primitive,” writes Fitzgerald. “Like the young boys who play with guns and explore their sexuality, Clark’s drug users plumb the depths of rapacious desire, so repressed and unexplored in the modern body. Clark’s lifework is to bring this primitive desire to light in a liberal artistic adventure.”
Clark wasn’t the only photographer to represent heroin users this way. Documentary photographer Eugene Richards' 1994 book Cocaine True, Cocaine Blue focused on cocaine use in three inner-city neighborhoods. The book’s cover features an extreme close-up of a woman clenching a syringe between her teeth.
The image is arresting and also influenced the way many other photographers have depicted drug users to this day.
Photojournalists working for news agencies such as AP, Getty Images and The Denver Post have recently followed Richards' example and composed images of drug users with syringes in their mouths. In most of these photos, the heroin users' eyes are either partially or completely out of frame or hard to make out in detail.
It’s vital that photographers find more balanced ways of representing drug users, instead of reproducing the same types of stigmatizing images that have existed for decades.
Shocking images certainly provoke reactions. But it’s more important to offer context in order to spark discussions about solutions.
Hearing from the heroin users
In my own effort to produce and share balanced and humanizing images – and to reduce the possibility of misinterpretation and “othering” – I realized the images on their own couldn’t tell the full story. I needed a way to provide context for the viewer.
“The multitude of meanings in a photograph makes it risky, arguably even irresponsible, to trust raw images of marginalization, suffering, and addiction to an often judgmental public,” write Philippe Bourgois and Jeffrey Schonberg in their 2009 book Righteous Dopefiend. “Letting a picture speak its thousand words can results in a thousand deceptions.”
After selecting my final images, I showed them to Marie, Cheryl and Johnny. I wanted to know if they thought the photos accurately represented them, if they thought anything was missing and what they would have done differently if they had taken the photos themselves.
Many of their responses were positive. They thought that in most of the images, I’d accurately represented them. And they had important suggestions. Most of all, they wanted to be seen in the photos as more than just drug users.
I’ve included their most telling comments alongside each of the photos in this story.
A needle in my arm is only ten percent of who I am. The other parts are going to the park and playing, having fun outside and watching children play. Being as much a part of as I can be in the community. I’m not just some dirty, mistrusting, drug addict from the skid row.
I don’t have to be in alleys [injecting heroin] anymore, like I used to be. I’m in a safe environment, no risk of getting or transmitting any infections, and my health is taken care of.
I’m caring for my pet whom I’ve have taken on the bus…I’m not selfish…. I don’t just think of me and my addiction. That was me, on the bus, going to see my Mom. I was going overnight so I had to take my cat with me. There’s more to my life than addiction… Like my cat. Like my family. Like taking time out to remember where and who I truly am. And where I come from.
People looking at this photo might possibly see that I’m being cruel. Which is not what I want them to see. I wasn’t trying to hurt her. She looks very scared and sad there. She looks alone. And I don’t like that because she’s not. I wasn’t trying to hurt her. I wanted her to meet my mom.
People seeing this photo could think anything . They could think that I’m going to see a drug dealer, they could think basically whatever they want, but that’s not what it is. I was going to see my Mom. [I wish viewers could see] my face, the smile on my face that I’m happy to see her. The excitement that I had because it was the first time I had seen her in a while.
I look confused, maybe a little freaked out or something. I don’t like [the photo]. I wish it weren’t so close up. Maybe it’s a harsh truth, I don’t know.
People seeing this photo might see somebody who’s happy, somebody who isn’t so dark or depressed…somebody who’s carefree and playful, and likes to enjoy herself. I do that all the time. I’m always like that… With a smile on my face, I try to always be happy. Which is really hard sometimes but yeah… It’s me.
I would like it if maybe they’d let me comb my hair, instead of looking like a real hardcore junkie here. I didn’t realize my hair looked so bad when I take my shirt off.
The reason why I take my shirt off is because I muscle the dope, I don’t IV it, because the reason why I do the dope is different from why a lot of other people do it. They do it to get high, I do it to help with some pain issues I have. I don’t want people thinking, “You know, these guys are going in there taking our tax dollars and doing heroin and getting high, look at them. You know, they’re nothing but detriments to society.” Well, I’ll tell ya, it’s saving my life.
I have a love for animals, especially cats. I had a cat in my life for the last year-and-a-half…well, no, the last eight months. And the more time I spent with humans, the more I love my cat.
I’m not much on being a show off, that’s why I put [the Siberian tiger tattoo] on my back… It’s something I’ve always wanted to do … and I managed to do that.
In this photo I’m trying not to break the law and grab some bottles and cash them in. So I can basically eat and have food. What’s missing is the security guards who usually hassle me. And, they have no reason to because I’m not hurting or stealing from them.
I’m also helping the environment because 80 percent of these bottles end up going to the landfill or the garbage. It’s not good for our ecosystem.
At this point in my life, I feel like I could come home at night and look in the mirror and not feel guilt or shame for what I was doing out there. Because I’m not stealing from anybody or hurting anybody.
People looking at this photo will see a fella who looks very intense. He looks tired. He’s out trying to make an honest dollar. He’s not proud of what he’s doing. But he’s doing what he has to, in order to survive. At the point where I’m at in my life, I think it’s a 100 percent accurate description of where my life is at. You can see the weariness, the life, the trials and tribulations I’ve been through.
I used to go into the shops and shoplift. I shoplifted quite a bit of food from this shop to feed my drug addictions, and that’s one thing you don’t see in this picture right now. I came and stole from this place and yet, a year later, I’m welcome to come in that store because I made an immense change and do not steal in there now. I come in and buy food like any other individual, and it makes me so proud to be able to do that.
You can see the intenseness in my face. It looks like I’m thinking deep about something and it’s just a feeling of gratitude of being happy and being alive… I hope people get out of this photograph that it’s never too late. And what I’ve been through in my life. We always have a chance as long as we stay positive in the moment. Live in the moment.
These are some nice carvings. If you look close enough, done in jade. Very nice done little pieces and very expensive little pieces.
This photo represents a point in my life when I needed money to do dope. These were the things I would steal to feed my drug addiction. And they were small enough, and easy enough to steal that I would do it. And I had no problem doing it. I never once got caught stealing and grabbing these pieces of ornaments. I would go into the store and take about five minutes. Five minutes of work would keep me unsick for approximately two or three days.
People viewing this photo might see some young girl, downtown, in a back alley. Looks like it’s a rough alley. A young girl, maybe she’s strung out, or maybe she’s determined to find drugs or who knows what they see in this photo. They just see a young girl smiling and looking down the alley.
Yeah, it shows all of me. I just hope the people see me in this photo – that I’m a striving, struggling drug addict. That I’m trying to better my life.
I want to show the people that this place is where we get our injections for our heroin opiate program, just show them that we need these places so heroin addicts can get off the streets. Heroin can be contaminated with many different poisons out there that can severely give us infections, because they put hog dewormer in the heroin on the streets. The clinical heroin here, there’s no bad chemicals or poisons in the drug. It helps us through the day, takes our aches and pains away, everything that heroin used to do.
In other places of the world, they had this study and it’s helped them, that’s why they brought it to Canada, here to [British Columbia]. And for us, the people who are in it, we’re so lucky and should be so grateful to have such a great program.
I hope the people see through this documentary all the points, all the emotions and desires, needs, and wants that we need, that you can help us down the road be able to successfully show our governments that people need the extra bit of help because we can’t do it on our own.
We need for you people to see that we’re not stereotyped monsters. We’re people just like you, just with an addiction. Something that we do a little bit more than others… When you look at this, take it with a grain of salt, because it could be your own daughter, it could be your own son out there doing exactly what I’m doing, but they had the door closed.
A drug addict’s world is not just the drugs, it’s how they get them, what you gotta do to get them. Sex trade, you know. Stealing, killing, whatever it might take just to get that extra dollar to get that extra fix so you can feel numb for the rest of the day. Not necessarily it’s always that, but in my life, I just want you to know that I’m struggling and I need that extra help.
I think the people will see a young girl having a cigarette out in the rain, painting her fingernails, enjoying the weather. Really studying, “Oh, come on, get the last bit of that nail polish out of the bottle.” I am just on the outside in the rain. I’m content. I’m puffing on my cigarette.
Well, now people will see that I have a band aid on my hand. They might think she has a cut on her hand, that’s why she’s having difficulties painting her fingernails and getting that nail polish out of the jar.
I’m sure there’s hundreds of photos that could show my life different. But my life today is a recovering heroin addict. I’m 124 pounds. I used weigh 97 pounds. There’s so many good things, and positive ways of looking at my life. If a picture could show all that emotion in one? That would be great, but it won’t and that’s all that my voice could tell you.
I think that people see a girl looking in the mirror, looking in fear, like what is she doing with the needle in her neck, sticking in her neck, that’s a pretty dangerous site to be injecting. But that’s the reality of that picture. It’s me being all strung out on dope, trying to get that shot into me, and it’s filled with blood and I’m trying to plug it into my vein cause I need that drug that’s in there so I can get off and get high, numb whatever pain I’m going through in that moment.
I was all fucked up on drugs that day, yeah. It shows my emotion, my fear, my determination. [I wish the photo had] maybe a little bit more light… Just to show it’s hard to inject into your neck like that. Just to show the picture more. To see what kind of struggle it is to inject in your neck. And to show maybe just a little bit more emotion to the people just to show what and why I’m doing that to myself.
Postscript: depicting the lives of users
Throughout the project, I’d spoken with the subjects about the purpose of the photo essay – to challenge the stereotypes of drug genre photography and to help spread awareness about heroin-assisted treatment.
I often explained to them that their photos would likely be published on the Internet – that police, future employers and others could learn they are heroin users. Despite the risks, the three subjects reiterated that they wanted to take part in the project because they, too, wanted to tell others about heroin-assisted treatment.
I’d been told that after enrolling in the heroin-assisted treatment study, some participants had reconnected with family members, found stable housing and gotten jobs. I hoped that I’d be able to take photos of Marie, Cheryl and Johnny in these types of settings.
However, I quickly learned that this wouldn’t be easy. Two of the three subjects didn’t engage in many other activities beyond self-injecting at the Crosstown clinic three times a day. Outside the clinic, much of their time was spent acquiring and using drugs.
This meant the moments I was able to capture ended up being far less varied than I’d anticipated.
Still, there were revealing moments, like when I managed to photograph Marie traveled across the city by bus to try to find her mother. It was Thanksgiving and she hadn’t seen her mother in over two years. I thought these particular photos might help the viewer understand Marie in a new way: even if people weren’t able to fully understand the depth of Marie’s suffering or the roots of her addiction, everyone knows what it’s like to want to spend the holidays with loved ones.
The greatest challenge I faced was determining how to document two of the subjects' ongoing drug use outside of the heroin-assisted treatment study. I simply couldn’t ignore it because it was a major part of their day-to-day lives. Marie and Cheryl told me that since the study was double-blind, they might not have been receiving the right medication – or high enough doses – to suppress their need to use other drugs. This doesn’t mean heroin-assisted treatment doesn’t work.
When the time came to choose the final photographs, I deliberately left out images that I suspected could be viewed as the most sensational or degrading.
My photo of Cheryl, lit by a candle and injecting drugs into her neck in front of a mirror in her apartment may not appear any less shocking than other drug genre photographers’ images of injection scenes.
However, Cheryl’s own words that accompany the photo provide critical context for the viewer. She explains that she was compelled to buy street drugs and inject into her neck – even though she knew the drugs could be contaminated and possibly kill her – because she was desperate to do whatever she could to feel well, even if this meant risking her life.
In order to see Cheryl as more than a drug user, the viewer needs to know this.
If death is the final taboo, it might not be for much longer. There has, in recent years, been increasing effort to promote conversations about death and dying, both in the home and in more public settings. For example, death cafes, first launched in Switzerland in 2004, have spread around the world, enabling people to speak about their fears over cake and coffee.
Our reluctance to talk about death is often taken as evidence that we are afraid, and therefore suppress thoughts about it. However, there is little direct evidence to support that we are. So what is a “normal” amount of death anxiety? And how does it manifest itself?
Experimenting with death
Judging by studies using questionnaires, we seem more bothered by the prospect of losing our loved ones than we do about dying ourselves. Such studies also show that we worry more about the dying process – the pain and loneliness involved, for example – than about the end of life itself. In general, when we are asked if we are afraid to die, most of us deny it, and report only mild levels of anxiety. The minority who report high levels of death anxiety are even considered psychologically abnormal – thanatophobic – and recommended for treatment.
On the other hand, our tendency to report only low levels of death anxiety might be a result of our reluctance to admit to our fear, to others and ourselves. Based on this hypothesis, social psychologists have, for almost 30 years now, examined the social and psychological effects of being confronted with our own mortality. In well over 200 experiments, individuals have been instructed to imagine themselves dying.
What’s worse: the death of a loved one or facing our own death? (image: Photographee.eu)
The first study of this kind was conducted on US municipal court judges, who were asked to set bond for an alleged prostitute in a hypothetical scenario. On average, judges who were confronted with their mortality beforehand set a much higher bail than those who were not confronted – $455 versus $50. Since then, many other effects have been found among groups including the general population in many different countries.
Besides making us more punitive, thinking about death also increases our nationalistic bias, makes us more prejudiced against other racial, religious and age groups, and leads to other such parochial attitudes. Taken together, these dozens of studies show that being reminded of death strengthens our ties to the groups we belong to, to the detriment of those who are different from us.
Reminders of death also affect our political and religious beliefs in interesting ways. On the one hand, they polarise us: political liberals become more liberal while conservatives become more conservative. Similarly, religious people tend to assert their beliefs more fervently while nonreligious people disavow more.
On the other hand, these studies have also found that thinking about death tempts us all – religious or otherwise – towards more religious belief in subtle, perhaps unconscious ways. And when the reminder of death is sufficiently powerful and when participants are not mindful of their prior political commitments, liberals as well as conservatives tend to endorse conservative ideas and candidates. Some researchers claim that this could explain the US political shift to the right after 9/11.
What do the results mean?
But why does the prospect of death make us more punitive, conservative and religious? According to many theorists, reminders of death compel us to seek immortality. Many religions offer literal immortality, but our secular affiliations – such as our nation states and ethnic groups – can provide symbolic immortality. These groups and their traditions are a part of who we are, and they outlive us. Defending our cultural norms can boost our sense of belonging and being more punitive against individuals who violate cultural norms – such as prostitutes – is symptom of this.
Consistent with this interpretation, researchers have also found that reminders of death increase our desire for fame and for children, both of which are commonly associated with symbolic immortality. It turns out that we do want to be immortalised through our work and our DNA.
Thinking about death makes us dream of being famous. (image: Andrea Raffin)
When asked, we do not seem, perhaps not even to ourselves, to fear death. Nor would we guess that thinking about death has such widespread effects on our social attitudes. But there are limits to our introspective powers. We are notoriously bad at predicting how we will feel or behave in some future scenario, and we are similarly bad at working out why we feel the way we do, or even why we have behaved a certain way. So, whether we realise it or not, it seems that to bring death to the surface of our minds is to open Pandora’s box.
So what should we make of these new efforts to demystify death and dying through conversation? It is hard to say. Increasing death’s profile in our imaginations, private and public, might make us all more punitive and prejudiced, as the research found. But then perhaps we get these negative effects precisely because we are unaccustomed to thinking and talking about death.
In exposure therapy, carefully exposing patients to the source of their anxiety – an object, an animal, or even a memory – reduces their fear. In the same way, perhaps this most recent taboo-breaking trend will inoculate us psychologically, and make us more robust in the face of death.
In the early years of my clinical practice as a psychologist treating heroin users, I commonly saw adolescents and young adults using heroin as their first drug. A typical client was a male in his mid-teens, perhaps a runaway or living in foster care, or someone who had been in and out of juvenile detention, or dropped out of school and who was court-ordered into treatment. When we saw older heroin users in treatment, it was considered unusual. That’s not the case anymore.
According to a new study, 50-59-year-olds are the largest age group in opioid treatment programs. Another recent study found that drug overdoses were a factor in the rising mortality rate for non-Hispanic white middle-aged Americans.
According to reports in the Journal of the American Medical Association, the new generation of heroin users is older, predominantly white and living outside of inner-city urban neighborhoods. And the average age of first heroin use has increased from age 16 to over 23 and from equal numbers of white and nonwhite users to about 90% white.
Why have the demographics of heroin use changed so much? For that, we can look to dramatic increase in prescriptions for opioid painkillers, such as Oxycontin or Vicodin. These medications can treat acute and chronic pain, but can also lead to addiction. And when people can’t access pills anymore, heroin can provide a cheaper and more powerful alternative.
Overdose deaths are up
The incidence of drug overdoses is five times higher today than 35 years ago. In 2009, drug overdose deaths passed motor vehicle deaths for the first time. And prescription pain medications, specifically opioids, have increasingly accounted for the majority of drug overdose deaths.
From 1999 to 2010, drug overdose deaths from opioid pain medications increased from about 30% to over 60%, and in 2010, the most recent year that statistics are available, deaths from opioids far exceeded deaths from any other legal or illegal drug class.
In large part, this increase stems from a change in how doctors treated pain that began in the 1990s. At that time, I was working in a large, urban hospital system, and both researchers and clinicians were advocating aggressive and proactive treatment for pain. Restrictions on prescribing opioids were lessened, and physicians were being encouraged to more adequately treat their patients’ pain.
And prescriptions for opioids have gone up dramtically. The Centers for Disease Control and Prevention (CDC) reports that as recently as 2012, over 250 million prescriptions for pain relievers were written in the United States per year, representing a 300% increase in the previous 13 years.
Unfortunately, with the increased use of prescription opioids, there was a commensurate increase in overdoses.
Why are more older people becoming addicted to painkillers?
The National Institutes of Health reports that chronic pain patients tend to be older, that their pain is of longer duration, more often accompanied by other conditions and more likely to be treated. For patients in severe pain, opioids are often the only effective treatment.
There are three primary effects of opioid use: analgesia (pain relief), sedation and euphoria. Patients experience the three differently, depending on their reasons for using the drug. Some people may become dependent on opioids, and some will become addicted – and they are not the same thing.
Dependence is defined as having withdrawal symptoms when the drug is stopped, while addiction is the compulsive use of the drug for a state (euphoria) other than pain relief. The compulsion becomes so consuming that the addict’s life centers around seeking and obtaining the drug, using it, withdrawing from it and seeking it again, to the neglect of all other aspects of life.
While opioids carry the risk of addiction, not all patients will become addicted. For example, patients being treated with opioid medications after surgery are not likely to become addicted, regardless of the dose. That is because for the postsurgical patient, the sedative and analgesic effects of the medication override the euphoric effect.
On the other hand, individuals who focus on the state of euphoria (the “high”) are the ones more likely to become addicted.
How does abuse start?
As clinical psychologist working with pain patients over the years, I was able to observe distinct patterns of use. Some people were able to stop the pain relievers with relative ease after recovery. Others might start taking opioids for nonmedical reasons.
Here’s a typical example: a patient who had been prescribed Vicodin after back surgery might need fewer pills after a while to manage their pain, but was afraid to tell the doctor (“What if the pain comes back?”), so the prescriptions continued. By the time recovery was complete, the patient had a stockpile of pills. One day after work, this patient came home with a headache from a stressful day. In the medicine cabinet were the leftover Vicodin. A couple of pills, and the patient experienced relief not only from the headache but from the stress of the day. The next time, taking the pills was easier, until before long, the patient was addicted and seeking more. This patient, like many who become addicted, did not intend to start abusing the drug.
Eventually, the prescriptions stopped, but the addiction did not, and many of these patients either began to doctor-shop, a term that describes frequent changes in doctors or having multiple doctors in order to obtain prescriptions, or they turned to illegally obtained drugs, prescription or street drugs such as heroin.
Heroin is cheap. A single 80mg OxyContin pill can cost between US$60 and $100 on the street, compared to $45-$60 for a single purchase of multiple doses of heroin. Heroin also has a larger effect, depending on the purity and method of ingestion, and doesn’t have the ceiling effect that controlled prescriptions have.
Data from Substance Abuse and Mental Health Services Administration (SAMHSA) back that up. SAMHSA reports that nearly 80% of heroin users report having become addicted to prescription pain medications first, while just 3.6% had a history of heroin use before beginning prescription pain medications. Heroin is now rapidly replacing Vicodin, Oxycodone and other prescription opioid painkillers as the drug of choice for nonmedical use by a growing population of users.
And there are reports that drug dealers may encourage drug seekers to use heroin, if they cannot afford prescription medicines. As more older people become addicted to opioids, more may turn to heroin.
A study of heroin users conducted by researchers at Washington University in St Louis, Missouri reported that typical heroin users in their study were white, middle-aged, and equally divided among males and females.
When asked about switching from prescription pain medications to heroin, many reported that they felt forced to switch because of lack of availability of the prescription drugs.
Can policy fixes turn the tide?
In an effort to curb the rising rates of addiction to prescription opioids and the associated costs in lives, the US Drug Enforcement Administration (DEA) has imposed restrictions on the prescribing of hydrocodone combination product, like Vicodin.
These include strength, number of doses, frequency of prescription and method of delivering new prescriptions.
While attempting to curb the nonmedical use of the opioids, these policies are also limiting access to pain treatments for the legitimate pain patient. However well-meaning these new laws are, it remains to be seen whether or not they will force increased numbers of pain patients to the streets and street drugs for relief.
In the meantime, physicians would do well to learn about opioid use as well as engage in drug screening and monitoring, pill counting and the use of other pain management protocols such as behavioral counseling. That would be an important beginning of the end of the drug addiction cycle.
The weather might seem like it creates weeks of dreary, grey drizzle. But it can also put on a truly sensational – and, often, deadly – show. But what explains these explosive events?
The Earth’s atmosphere is driven by heating from the Sun. Weather is the response of the atmosphere to the uneven pattern of heat energy that it receives. Visible and ultraviolet light warms the Earth during the day, more strongly at low latitudes, but the Earth emits an almost exactly equal total amount of infrared radiation in all directions.
On average, the Earth receives 340 W m-2 from the Sun. About one third of this energy is scattered straight back into space by clouds and ice on the surface. The remaining energy, roughly the equivalent of placing a small radiator every 2m in a lattice covering the Earth’s surface and running them continuously, is absorbed by the surface and atmosphere.
The Earth’s temperature does not show extreme variations, varying by less than 50° C between Equator and high latitudes, much less than on a body such as the Moon. This is because the atmosphere (and to a slightly lesser extent the oceans) transports heat from warmer to cooler regions. Atmospheric heat transport peaks at about 5 PW (5 petaWatts or 5 × 1015 W). For context, the largest nuclear power station has a capacity of 8 GW (8 × 109 W) and the total power consumed in all forms by humans today is estimated to be 18 TW (1.8 × 1013 W), over 250 times less.
This vast power supply is what drives the heat engine of the Earth’s atmosphere and oceans, and the resulting motions of warm air to cooler regions. Along the journey, energy is transformed into many other forms and the rotation of the Earth has a profound influence on the form the weather takes, especially at middle latitudes. Here the prime means of heat transport changes from the longitudinally-symmetric over-turning Hadley Cells to wave-like motions, the surface manifestation of which are our familiar high and low pressure weather systems.
1. Jet Streams
Jet streams are very narrow ribbons (a few km deep and maybe 100km wide) of fast moving air that circle the Earth and form on the boundary of warmer and colder air masses at about 10 km altitude. In the core of a jet stream, winds can reach 200 km hr-1 and an amazing 656 km hr-1 has been recorded over the Outer Hebrides in December 1967. The location of these focused winds is vital to planning aircraft routes and clever use is the reason why it is faster to fly from west to east than the reverse journey.
A band of cirrus clouds produced by a jet stream. (image: LPI/NASA)
The jet stream that most influences our weather is the northern polar jet stream which meanders in a varying route and guides the passage of weather systems around the globe, potentially leading to a series of storms and flooding. When the jet stream curves south then cold polar air will be brought down, when it curves to the north, warm air and settled weather may result.
2. Tropical Cyclones
Tropical cyclones, better known as hurricanes in the Americas and typhoons in the Far East, are massively destructive weather events that at lower latitudes, begin as weaker, low-pressure weather systems. Tropical cyclones form over very warm seas, typically in late summer and autumn in each hemisphere. As they intensify they become driven by latent energy release from water vapour, which condenses to form the high storm clouds.
Wind speeds of over 200 km hr-1 have been recorded around the centre of a storm, but devastation is mainly caused by flooding as a result of the surge in sea surface height and the intense rainfall. The average UK annual rainfall may fall in less than two hours from the clouds around the eye of the storm.
Hurricane Katrina at peak intensity in the Gulf of Mexico on 28 August 2005. (image: NASA)
The 1970 Bhola cyclone was one of the worst natural disasters of all time, killing half a million people in Bangladesh and West Bengal largely as a result of such flooding, but it was far from the most powerful tropical cyclone, rating a relatively moderate Category 3. The strongest, Category 5, storms include Hurricane Katrina in 2005 with winds of over 280 km hr-1.
3. Tornadoes
Tornadoes are smaller, violent whirlwinds that can form below a cumulonimbus storm cloud, a region of intense vertical convection. A funnel cloud forms in the centre of the vortex, although the strong winds circulate much further around it. The most extreme winds are almost 500 km hr-1, and result in extreme damage along their path.
An occluded mesocyclone tornado. (image: NOAA/Flickr)
The Tri-State Tornado of March 1925, had the longest path length recorded at over 350km and killed 695 people in the Mississippi River Valley, US. It was part of an outbreak with a combined death toll of 747, but even that was exceeded in April 1989 by the Daulatpur–Saturia tornado in Bangladesh, when more than 1,300 people died and 80,000 were left homeless.
4. Dust Storms
Dust storms occur in many parts of the world and can transport sand and finer mineral grains from one continent to another. In North Africa these storms are known as haboobs and are often initiated by the high winds associated with thunderstorms. Similar storms occur in the drier parts of the Americas and Asia. Haboobs can reach heights of more than 1km, cover thousands of km2 and last for hours, the lofted dust absorbing sunlight, warming the air and intensifying winds at the storm’s edge.
A dust storm heading for Mungerannie Hotel in South Australia on January 31, 2010. (image; Sydney Oats/Flickr)
On Earth, water droplets will nucleate on the finer dust grains, eventually removing them and limiting the growth of a storm, but on Mars, which is much drier, some dust storms can eventually cover the planet.
5. Dust Devils
Dust devils are small convective vortices, made visible by the dust that they lift from the surface. They are also driven by heat energy, where a cooler atmosphere is in contact with a warm surface. This is most common in desert-like regions, but they can happen even in temperate climates and there are recordings of “snow devils” on brightly-lit mountainsides.
Lightning is a common phenomenon in Earth’s atmosphere, occurring in regions of strong vertical convection. About 2,000 thunderstorms are active at any moment. Air in the narrow centre of a lightning channel can briefly reach 30,000°C, five times the temperature of the surface of the Sun.
Lighting off of Miami Beach. (image: Jussi Ollila/Flickr)
The thunder sound comes from the rapid expansion of the heated air and trees that are struck are literally blown apart as water within them instantly boils.
7. Hail
Hail is generally associated with thunderstorms and is also a warm weather, convective phenomenon. People often regard hail as a winter event, but late spring and summer is the only time that true hail occurs in the UK. When there are strong updrafts of air, hailstones can reach very large sizes, up to 20cm in diameter, and can weigh almost 1 kg.
Hail stones over 2" in diameter fell across 2 miles of southwest Oklahoma. (image: State Farm/Flickr)
Hail storms can be truly deadly and sadly there are records of many hundreds of deaths. Possibly the deadliest hailstorm recorded killed more than 230 people and 1,600 livestock in Uttar Pradesh, Northern India in April 1888, and there are written records of fatalities in Warwickshire, England as far back as May 1411.
As e-cigarettes become more popular, there has been a push to understand whether they are a “gateway” to regular, combustible cigarettes.
Two recent studies on e-cigarettes as gateways to smoking in teens and young adults have made headlines. And opponents of e-cigarettes have welcomed any crude signal of gateway effects.
As a publichealthprofessorwithrelatedresearch and interests in tobacco policy as well as in the complex factors that influence use of tobacco/nicotine products, I want to offer some thoughts on this research. Looking for a gateway effect between e-cigarettes and smoking is understandable. But is it the best question to ask about e-cigarette use?
The studies
These studies find evidence for a small association (or limited gateway) between e-cigarette use in nonsmokers and a progression to trying cigarettes in a one-year study period.
The more recent of the two studies was published in September 2015 (authored by Primack et al), in JAMA Pediatrics. Researchers followed 694 12-26-year-olds for a year. None had tried cigarette smoking at the study’s start, though 16 had tried e-cigarettes. (Perhaps the worthiest headline would be that only 2% of never-smokers tried e-cigarettes.)
A year later, 10% of the never-triers of e-cigarettes had taken at least one puff on a cigarette. But 38% (six of 16) of e-cigarette triers had taken at least one cigarette puff. This study focused on cigarettes and reports no information on prior hookah, cigar, marijuana, alcohol or smokeless tobacco use. If even two of the 16 were discounted because of prior use of other products, these results would likely be statistically insignificant.
The other study (authored by Leventhal et al) was published in August 2015 in JAMA. They followed 2,530 14-year-old school students for one year. None were smokers of any combustible tobacco products, including cigars, hookah and cigarettes at the start of the study, but 222 had tried e-cigarettes.
After 12 months, 25% of the e-cigarette triers had smoked at least one puff of a smoked tobacco product, compared to only 9% of the non-e-cigarette triers.
‘At least one puff’
Both studies found that young people who tried e-cigarettes were somewhat likelier to try smoked tobacco products, but that doesn’t mean e-cigarettes are a substantial gateway to regular smoking.
Rather than reporting usual measures of current smoking (ie, any cigarettes in the past 30 days) or daily smoking, both studies used “at least one puff” or “just a few puffs” in the past six months or lifetime.
It is as if an apple researcher thought “taking at least one bite of an apple in the past six months” was an important measure of initiation of apple eating.
But, research shows that a puff on one cigarette is crudely linked with daily smoking. Following teenagers who had not yet puffed on a cigarette, they found that 48% took at least one puff in the 12-month follow-up period. But of those, only 20% became daily smokers.
Leventhal et al do acknowledge that future work needs to assess risks of “regular, frequent” smoking. Indeed, until we understand if the observed small gateway is only to experimentation or to frequent, dependent smoking, the more critical question is unanswered. In that only a subset of these observed gateway triers will move on to be regular smokers, it is almost certain that further follow-up of these samples will be unable to demonstrate a major gateway to heavy tobacco use.
Both studies also used a measure of “susceptibility” to smoking that is even more tenuously connected to becoming a future frequent smoker and also can be greatly discounted by assessing prior use of other drug products, including smokeless tobacco.
The gateways that aren’t
The observed gateway effects in these studies at best indicate some small increased chances of future smoking for the minority of these e-cigarette triers – not large, inexorable movement toward cigarettes for the majority. In fact, drug research has generally turned away from the scientific usefulness of causal drug gateway models.
Gateway models began in the 1950s when drug enforcement authorities warned that marijuana use caused deadly heroin use, which has not been found to be true.
Just as trying beer and liking it (or not) might incline one to try liquor (or not), prior use of one nicotine product can influence use of other nicotine products.
Drug research emphasizes so-called “common liability models” in which personal and contextual factors are taken into account as determinants of use or nonuse of products. While “products” themselves can influence the likelihood of using other products, it is important to consider “persons” as a factor determining use.
For example, if religious beliefs contribute to some teenagers not drinking alcohol, not smoking cigarettes, not using e-cigarettes, and at the same time lack of religious beliefs incline other teenagers to do these things, one would see an association between using these various products. Such an association is caused both by factors that influence nonuse of products as well as factors that influence use.
While these studies both attempted to different degrees to control contextual and personal factors that could be linked to smoking, this is easier said than done. The study from Leventhal et al does try to control for the use of alcohol, marijuana and smokeless tobacco (another nicotine product), but uses only one two-level measure of “any use” versus “no use” of all these products. Blunt tools lead to cruder results.
Science aside, gateway rhetoric has long been an important political tool. Fears that e-cigarettes are gateways to smoking are being used to justify policy or regulations. Yet, arguments for product regulations can be made forcefully, without needing to wave the gateway flag.
Let’s flip the question these studies asked. Instead of only asking whether nonsmoking e-cigarettes users move to smoking, why not explore whether higher-risk e-cigarette triers who have also tried smoked products are prevented from becoming established smokers? Such a question surely needs better than the “one puff” measures of product usage and recruitment to smoking.
Leventhal et al found that 75% (the large majority) of baseline e-cigarette users did not smoke at 12-month follow-up, compared to 91% of nonusers of e-cigarettes. But we don’t know how many smokers who tried e-cigarettes in these age groups were still smoking (beyond a puff) in the future. By the limited logic of the current gateway research, patterns of reduced smoking for e-cigarette users compared to smokers could be interpreted as evidence of preventive effects.
What research should we be doing?
The tobacco and nicotine products are often already illegal for youth to purchase. But these products are legal for adults. The focus on minor gateway effects for youth should not distract from the need to explore policy and clinical questions about harm and disease riskfrom adult use of legal tobacco products.
Cost, convenience, perceived risks (and official messages about risks) as well as personal preferences can influence which among many products are most used.
It is important to understand interrelationships in tobacco/nicotine product use by adolescents and adults, but both the questions and measures need to be broadened. In addition to concerns for lower-risk youth, we need to assess patterns of product use in higher-risk youth who have tried multiple drugs (alcohol, marijuana, cigarettes, cigars, smokeless tobacco and hookahs) and often have mental health issues. We need to understand how best to prevent these youth from becoming regular users as adults of deadly smoked products.
Last November, the Board of Health for Westminster, a town in central Massachusetts, proposed prohibiting all tobacco sales – even e-cigarettes – in the town.
Westminster’s three-person Board of Health said that the proposal was meant to protect the next generation from tobacco and nicotine products. The board expressed frustration at its inability to keep up with the seemingly endless barrage of new tobacco products that appealed to minors. Ending all tobacco sales seemed like a clean and quick fix.
But in the face of intense opposition, Westminster’s Board of Health voted to drop the proposal. While banning tobacco sales might have protected children, many felt the proposal infringed on the “rights” and “freedoms” of adults. Some also suggested that people would simply go to other towns to buy tobacco products.
In proposing to ban all tobacco sales at once, Westminster’s Board of Health got ahead of itself. But there are plenty of other strategies that cities and towns can use to effectively reduce tobacco use – especially in young people – that don’t go as far as a total sales ban.
These measures, while aggressive, might help diffuse complaints of “prohibition” and instead keep the focus on dramatically reducing the 480,000 deaths caused each year by tobacco products. And, critically, these policies avoid the pitfalls that doomed the Westminster proposal.
To protect kids, make it harder for them to buy cigarettes
While tobacco sales to people under 18 are prohibited, most high school students report that they have little difficulty in gaining access to cigarettes.
There are two policy options that would make it a whole lot harder for kids to start smoking, while not preventing adults from buying tobacco products: raise the legal buying age to 21 and restrict cigarette sales to adult-only retailers.
Raising the age to 21 works because high school students get tobacco primarily from friends who can legally purchase tobacco. Ninety percent of those who supply cigarettes to minors are under 21. Raising the minimum sales age to 21 puts legal purchasers outside the social circle of most high school students.
A recent study found that raising the tobacco-buying age to 21 in the Boston suburb of Needham led to a nearly 50% decline in youth smoking, a much steeper decline than was seen in surrounding communities.
Obviously this helps prevent sales to minors. But raising the tobacco buying age doesn’t shield minors from tobacco advertising. Since other avenues of tobacco advertising (TV, billboards, sports sponsorships) have been sharply limited or prohibited, tobacco companies have focused nearly all of their advertising dollars on retail stores where tobacco is sold.
Limiting tobacco sales to retail locations that only adults are permitted to enter would remove this barrage of tobacco advertising from the convenience stores where teens spend a significant amount of time. It would also make it easier to prevent minors from purchasing cigarettes.
This is not a radical strategy; it’s similar to how liquor sales are currently regulated in most states. Ideally, limiting cigarette sales to adult-only retail outlets would be done in conjunction with raising the minimum buying age for tobacco from 18 to 21.
These policies wouldn’t prevent adults from purchasing tobacco, but they would help keep youth from taking up smoking (while also making it easier for current smokers to quit).
Focus on the most dangerous tobacco products
Westminster’s Board of Health proposal to ban the sale of all tobacco products also included e-cigarettes, which contain nicotine derived from tobacco. This struck many as radical and unwarranted.
The vast majority of all tobacco related deaths result from the use of only one particular product: the cigarette.
People use tobacco products primarily because nicotine is addictive. Nicotine itself is not benign, but on its own it’s much less harmful than the smoke and tar produced by burning tobacco. E-cigarettes and other vaporized nicotine products are almost certainly less toxic and less harmful when used instead of conventional cigarettes.
A bold yet more incremental step would be to allow the sale of potentially less harmful products, like e-cigarettes, while sharply limiting sales of conventional cigarettes and other combusted products. This might take the form of exempting e-cigarettes from the adult-only retailer policies described. Or, potentially, a community might consider prohibiting all cigarette sales, while allowing sales of non-combustible products.
If cigarettes were harder to come by, the “harm reduction” potential of e-cigarettes would be much more likely realized. As summarized by the Surgeon General:
The impact of noncombustible [e-cigarettes] on population health is much more likely to be beneficial in an environment where the appeal, accessibility, promotion, and use of cigarettes and other combusted tobacco products are being rapidly reduced, especially among youth and young adults.
But the evidence to date indicates that e-cigarettes are primarily being used along with cigarettes, rather than instead of them. In addition, use of e-cigarettes by youth, which is rapidly expanding, puts these youth in danger of “graduating” to cigarette use.
A recently published study found that adolescents who had used e-cigarettes were more than twice as likely as their peers to subsequently start smoking. Making it harder for adolescents to obtain cigarettes would help reduce the likelihood that minors using e-cigarettes move on to smoking.
Get community support before acting
The most important lesson of Westminster’s experience may be that policymakers cannot get too far ahead of their communities. As public health law scholar Wendy Parmet recently wrote:
Public health laws that are strongly rooted in, and indeed arise from, the public, may face a quite different fate than those that derive from the good intentions of public health policymakers alone.
Rather than announce a plan to ban the sale of all tobacco products, the Westminster board of health could have instead started a series of community discussions about the problem of tobacco use – and youth tobacco use in particular.
It is likely that such discussions would have quickly produced broad consensus about the need to better protect youth from tobacco, which could have then led to a discussion about potential policy solutions (such as those discussed above).
It is also notable that some of the loudest critics of the proposed Westminster law were proponents (and users of) e-cigarettes, many of whom struggled for years to quit cigarettes. Including this community in early discussions could have led to a shared vision about how to minimize the dangers of e-cigarettes while focusing on the much more significant harms caused by cigarettes.
Making sustainable public health policy requires the slow but important processes of community engagement, education, compromise, and consensus building. With deliberate and incremental steps to reduce the prevalence of tobacco in our communities, we can save countless lives.
There are surely social benefits to legalization. For one, fewer marijuana-related arrests should slow spending on the war on drugs, which has been astronomically expensive and unsuccessful.
And fewer arrests should benefit minority communities that have experienced racially biased drug-law enforcement. Blacks, for instance, face nearly four times the rate of marijuana arrests as whites, despite similar rates of marijuana use and overall drug usebetween the two racial groups.
Indeed, decriminalization doesn’t change the social conditions that sustain both marijuana use and racially biased responses to it. And decriminalization sidesteps the troubling links between marijuana, race and class that present problems much deeper than prohibition.
A Drug of the Oppressed
Cannabis – the plant that supplies marijuana – has a long history as a drug used primarily by lower social classes. Going all the way back to the 1500s, the vast majority of cannabis users have occupied socioeconomic margins: slaves, hard laborers, sex workers, prisoners and low-ranking sailors and soldiers. These people used cannabis to cope with the terrible conditions they experienced.
The origin of the word “marijuana” foreshadowed its current use. Historically, the earliest and most numerous group of users in the Americas were slaves from western Central Africa (modern Gabon to Angola). Their words for cannabis are now used in nearly all the places they (involuntarily) ended up during the 1700s and 1800s, which includes West Africa, the Caribbean and South America. Most notably, in Central America, the Kimbundu (Angolan) word mariamba became the Spanish word marihuana.
The slaves' vocabulary survived because people of all backgrounds valued the plant’s ability to help them cope with day-to-day lives characterized by hard labor, exploitation and trauma. Mariamba had the same mix of medicinal and recreational uses that it does today.
In fact, mariamba was only superficially African. It belonged, instead, to the transatlantic slave trade, an economic institution that linked five continents. In 1840s Angola (even when the slave trade was in decline), marijuana was primarily valued for “supporting the strength and condition of the slaves.” Central African slaves were smoking cannabis by the late 1700s, and introduced the plant to many locations by transporting its seeds.
Marijuana ultimately served the needs of exploited people; it was not intrinsically African. But because Central African slaves were in many places the first to introduce the drug plant, their cannabis culture widely dominated.
Importantly, few Central Africans ended up in the US, and those who arrived did not introduce drug cannabis or cannabis drug use. Marijuana entered the US only after 1900 because army privates and migrant laborers valued it, not because slaves brought it. (European colonists had planted hemp cannabis since the 1500s, but the European type of cannabis doesn’t produce mind-altering chemicals.)
Social class and race have been entwined for centuries. And because slavery, racism and segregation confined people of color to the lowest rung on the social ladder, cannabis use has been (incorrectly and stereotypically) tied to race for centuries.
But even a 2005 textbook used race to describe the drug’s introduction to America. “Hemp had been grown […] for a long time, but this had not led to an awareness of its psycho-active potential, at least in the white population,” the author wrote. “Black slaves, however, knew of it […from] back in Africa.”
Relying upon race to explain drug use clouds the social contexts that encourage drug use. And the people who first used marijuana in the US – which included all races, black, white or otherwise – were those confined to socioeconomic margins.
Despite periodic popularity in middle and upper classes since the 1960s, marijuana remains primarily a drug used by people at society’s margins. “Medical” marijuana serves people whose health-care needs aren’t met by mainstream institutions. “Recreational” use is most frequent among young, poor and unemployed people. Whether labeled medicine or recreation, marijuana has, for centuries, appealed to people coping with physical or mental stress (even if those difficulties might be shrouded in good vibes and giggles).
With the rates of legal and illegal drug use in the US – especially marijuana – higher than in most countries, it’s important for people to question and challenge the conditions that help perpetuate this dependence, and not just challenge the legality of one drug option.
Decriminalization might overthrow decades-long problems of prohibition. But it hardly acknowledges the centuries-long history of racism and elitism that has helped sustain marijuana use, and the biased responses to it.
What can be done? Society should explicitly link causes of marijuana use to the consequences of decriminalization. Decriminalized marijuana markets generate tax revenues. Some of this money should be spent to challenge institutional racism, by improving mental and physical health services in poorer neighborhoods and training police to avoid racial bias.
Marijuana is joining alcohol, tobacco and various prescription drugs as legal means for people to cope with the difficult realities of daily life. Right now, society has a brief opportunity to address meaningfully the social problems marijuana represents, and shouldn’t let this opportunity slip away.
When it comes to climate change, do you practice what you preach? While many of us express strong concern about the issue, there tends to be a yawning gap between this concern and many people’s willingness to actually act on it by doing things like using less power or petrol.
Why should we care about this “value-action gap”? Well for one thing, these practices can make a big difference: up to an estimated 20% of household emissions, according to one US study. Things like using housing insulation and public transport, if done on a wide enough scale, can seriously help the world avoid major climate change.
Many might attribute this gap to “cheap talk” – people say they care, but they don’t really. But survey after survey has shown that people are truly aware of the risks of climate change, and that it is a growing source of emotional distress. In Australia, national surveys in 2010 and 2012 showed that public acceptance and concern about climate change has remained very high, and that it is viewed as a genuine threat by many people across different ages, regions and income levels.
A much more disturbing idea is that people’s choices are shaped by their work and social settings, and that people’s lifestyles therefore hold them back from taking action. This is the crux of what the downshifting movement has been telling us about for decades: that your choices are not just yours alone, but are heavily shaped by the environment in which you live, the hours you work and play, and the social norms you embrace.
What time to adapt?
My colleagues and I re-analysed this extensive survey database, and found evidence to support this idea. Working conditions do indeed seem to influence the extent to which people act on their environmental concerns.
After controlling for a range of demographic variables and household income, we found that people who work longer hours tend to have a significantly larger gap between the extent to which they are concerned about the environment, and their actual engagement in environmentally sustainable practices.
It is tempting to attribute this to the effect of income – people who work longer are probably richer as well. But then again, wouldn’t more money make people better able to act on their concerns?
Here’s the catch: while the rich who declare themselves to be concerned about climate change do tend to buy environmentally friendly products, our results show they are also much less much likely to engage in time-consuming practices concerning how their goods are used, such as conserving electricity and fuel.
So what?
Our results suggest that policies to improve work-life balance and working conditions may deliver important environmental dividends. When it comes to adapting to climate change, governments and employers would do well to consider how long working hours can get in the way of environmentally sound behaviour.
Currently, millions of dollars are spent every year on public information and engagement campaigns to encourage the voluntary adoption of environmentally sustainable practices. Yet evidence suggests that such campaigns are relatively ineffective, partly because behaviour patterns are “locked” into existing lifestyles.
What’s more, as the economist Clive Spash has pointed out, standard “tax-and-subsidise” measures, such as both the carbon tax and the government’s Direct Action plan, are recognized to be both slow and costly to implement, and run the risk of reducing people’s motivation to take their own voluntary action.
In other words, there is a danger that the more people formally pay for carbon emissions, the less likely they are to do their bit to reduce their own carbon footprint.
Rather than narrowly focusing on taxing and subsidizing our way towards a more sustainable economy, we need to find way in which we can encourage people to act voluntarily on their environmental concerns. Rather than merely raising public awareness about climate change, the real challenge is to ensure that people have the broad capacity to respond to these messages.
Measures to improve work-life balance may help people to adapt their lifestyles so they can act on their environmental concerns.
The daily grind
For those of us caught in the daily balancing act between work and everything else, the advice is simple. Do take that opportunity to go home an hour early – not only are you safeguarding your mental health, you are also encouraging others to lead lifestyles that are more reflective of their values, environmental or otherwise.
Of course, if you go home and decide to burn coal for an extra hour, that’s not true.
But chances are that you, like most people, are concerned about climate change but just haven’t had the time to really think about what exactly you can do about it.
It’s time to change that – and that’s something that governments and employers, by implementing measures which promote a better work-life balance, can help out with too.
E-cigarettes and other vaping products are on track to out-sell cigarettes by the end of 2023. And more and more young people are trying e-cigarettes. So what do you need to know about them? Are they less harmful than using cigarettes or other burned tobacco products?
What are e-cigarettes?
First, they are not burned tobacco products. Most often, they contain nicotine solutions that are heated to make a vapor (hence the terms vape or vaping), and they’re usually powered by batteries. Some look like cigarettes and others can resemble flashlights. The first e-cigarettes were not produced by cigarette companies, but the cigarette companies have gotten into the business. E-cigarette and vaping products are available in specialty stores and convenience stores around the US with varying restrictions on purchase by youth under 18.
E-cigarettes don’t necessarily contain nicotine. Some popular products contain little or no nicotine and levels can vary from brand to brand. And nicotine isn’t always the reason someone might try e-cigarettes. In Canada – where nicotine-containing e-cigarettes are not approved, but still widely available – only 38% of adult cigarette smokers who also use e-cigarettes “always use nicotine” and 30% “sometime use nicotine” when vaping. And only 4% of those who never smoked tobacco reported using nicotine when vaping.
Why do young people use e-cigarettes?
A 2014 national high school survey finds more monthly vapers than monthly smokers: 17% of US 12th-grade students report using e-cigarettes in the past 30 days compared to 14% for tobacco cigarettes. We also know that patterns of infrequent, non-daily use of various tobacco and nicotine products may be increasing among young people. But trying e-cigarettes does not automatically lead to daily use.
Young people might also be influenced to try e-cigarettes because of how they are priced and promoted. They can be cheaper than traditional cigarettes and may be perceived as safer. Other features, like flavors can also supportuse in all age groups.
As e-cigarettes become more popular and more visible, young people will start trying and using these products. And because products keep changing, they will often try different kinds of e-cigarettes.
Youth is a time when individuals experiment with and get into trouble with psychoactive substances, including nicotine-containing e-cigarettes. In 2014, 44.4% of 12th-graders had ever used marijuana/hashish, and 35.1% had used in the past year; 41.4% reported being drunk in the past year. Users of one type of psychoactive substance are more likely to use others, like caffeine, alcohol, nicotine, THC or prescription drugs.
Is vaping safer than smoking?
The best evidence to date shows that using e-cigarettes is very dramatically less dangerous than cigarette smoking. Death from all causes within the ages of 25 to 79 is three times higher for smokers than never smokers. Compared to smoking, long-term health effects of e-cigarettes have been judged as likely “much less, if at all, harmful to users or bystanders.”
The 2014 Surgeon-General Report concluded that “The burden of death and disease from tobacco use in the United States is overwhelmingly caused by cigarettes and other burned tobacco products; rapid elimination of their use will dramatically reduce this burden.”
Recent reports suggest that vapers should be cautioned about how they use high-voltage devices because they can produce high levels of the carcinogen formaldehyde. But that, however, is not one of the common ways people use e-cigarettes. High voltage devices and long puffs can produce a bad taste that is avoided.
Burned cigarettes contain many carcinogens: the FDA lists 79 “harmful or potentially harmful” carcinogens in tobacco products and tobacco smoke.
Keep in mind that reports of a product being “not safe” in some way does not necessarily mean that it cannot overall be much safer than another product.
Are e-cigarettes a gateway drug?
The specter of some drugs being gateways to more dangerous drugs has preoccupied drug policy, and this is no different when it comes to tobacco products. E-cigarettes have been feared as possible gateways to cigarettes. If vaping has been acting largely as a gateway to cigarettes, one would expect to see more cigarette smoking with the rise in vaping. This has not happened. Smoking has continued to decline. Cigarette smoking by young people is the most powerful cause of smoking by adults.
In a broad sense, the world is full of products that can look like gateway products. The use of BMX bikes on dirt tracks by children could be gateways to the use of motorcycle dirt bikes by adults. But do the products cause the linkage or are individual tendencies more responsible for associations?
Much research on drug gateways supports a “common liability model” more than drug-based causal models. The Common Liability Model holds that characteristics (for example, liking to take risks) within individuals can be responsible for drug-use associations.
No matter whether you think (a) that trying of an e-cigarette is a causal gateway to later smoking that would not have otherwise happened or (b) that those who are more likely to try cigarettes are more likely to try e-cigarettes, once products become available to users, how these products are marketed influence which products are preferred. What is said and done about vaping can promote gateways to cigarettes. If you show more concern about vaping than smoking or if you downplay the deadly risks of smoking, you encourage young people to switch to cigarettes.
The policies that allow certain substances, like alcohol, tobacco and psychoactive substances, to be used quite freely by adults usually include prohibitions on use or purchase by youth. Without such policies, there might be even more experimentation by youth with these products. Prohibitions on sale of vaping products to youth should be supported.
What should you do if your teen smokes?
If you are faced with committed teenage smokers (who are probably also using other prohibited substances like drugs or alcohol), perhaps the best you can do is foster switching to e-cigarettes. Of course, do explore their interest in getting help with quitting smoking from quit-lines. For less-involved users of e-cigarettes who do not smoke regular cigarettes, encourage that regular use be avoided and that nicotine use be limited as much as possible.
Telling a teenager that vaping is just as bad for you as smoking or that e-cigs are worse than tobacco cigarettes could push them toward cigarettes and is not justified. It makes more sense to tell a young person that it is much better for their health if they stay away from tobacco cigarettes or cigarette-like tobacco cigars completely.
If you have teenagers who already both smoke and vape, encourage that they work to avoid cigarettes completely, and vaping could help them do so.
This article has been updated to correct mortality data for smokers.
With states legalizing marijuana by popular vote, some politicians, including Boston mayor Marty Walsh and New Jersey governor Chris Christie, are still calling marijuana a gateway drug.
The gateway theory argues that because heroin, cocaine and methamphetamine users often used marijuana before graduating to harder drugs, it must be a “gateway” to harder drug use. The theory implies that there is a casual mechanism that biologically sensitizes drug users, making them more willing to try – and more desirous of – harder drugs.
Yet the gateway hypothesis doesn’t make sense to those who use marijuana or have used in the past. Research shows that the vast majority of marijuana users do not go on to use hard drugs. Most stop using after entering the adult social world of family and work.
So why is it still part of the rhetoric and controversy surrounding the drug? A closer look reveals the historical roots – and vested interests – that are keeping the myth alive.
Explaining hard drug use
When analyzing what acts as a “gateway” to hard drug use, there are a number of factors at play. None involve marijuana.
With so much research challenging the gateway theory, it’s important to examine – and dispel – the research that proponents of the myth latch onto.
But what about all that evidence?
Most of the research linking marijuana to harder drug use comes from the correlation between the two. However, as any junior scientist can tell you, correlation does not mean causation.
Correlation is a first step. A correlation can be positive or negative; it can be weak or strong. And it never means a cause unless a rational reason for causality is found.
The brain disease model, which describes changes in the brain during the progression from drug use to addiction, currently gets a lot of attention as an potential causal link of the gateway theory. For example, in a 2014 article, neuroscientist Dr Jodi Gilman reported that even a little marijuana use was associated with “exposure-dependent alterations of the neural matrix of core reward systems” in the brains of young marijuana users. The reasoning goes that this would predispose them to use other drugs.
But other researchers were quick to point out the flaws of the Gilman study, such as a lack of careful controls for alcohol and other drug use by those whose brains were studied. Nonetheless, Dr Gilman’s research continues to be cited in the news media, while its critics are ignored.
In another study supporting the gateway theory, the authors admit to limitations in their study: that they excluded younger cocaine users from the analysis, as well as older cocaine users who had never used marijuana. This means that those cases that might provide evidence of no gateway effect were left out of the analysis.
One the other hand, there’s a wealth of research showing the flaws in the gateway theory. Unfortunately, the common thread among these studies is that much of them come from outside the US or from grass-roots organizations within the US that are promoting marijuana legalization.
A myth ingrained in politics, perpetuated through policy
So why is it that most of the funded research pointing out flaws in the gateway theory comes from overseas?
As Nathan Greenslit explained in an Atlantic article last year, US drug policy began with racist fear-mongering by Federal Bureau of Narcotics director Harry Anslinger in 1937.
The Nixon administration strengthened drug control with the creation of the Drug Enforcement Agency, which classified marijuana as a Schedule 1 drug, against the advice of the National Commission on Marijuana and Drug Abuse.
Because marijuana is still officially classified in the US as a Schedule I drug with no medical value, carefully controlled research using marijuana must receive approval from several federal departments. On the rare occasions that researchers do get approval, local politics can thwart the study.
Meanwhile, in the United States, addiction researchers and addiction treatment professionals are heavily invested in the weakly supported claim that marijuana is a gateway to hard drugs. For decades, scientists who study addiction have received millions in government and pharmaceutical funding to perpetuate the gateway hypothesis. Many would lose their respected reputations (or continued funding) if a gateway mechanism is not a legitimate research goal.
Today, what started as scare tactics under Anslinger has been “modernizied” (and mystified) by scientific jargon.
Sociologists Craig Reinarman and Harry G. Levine described how the media and politicians manufacture drug scares to influence policy. One fear perpetuated is that marijuana use will increase if decriminalized.
But a 2004 study compared Amsterdam, where marijuana was decriminalized, to San Francisco, where cannabis was, at the time, still criminalized. The authors found that criminalization of marijuana didn’t reduce use, while decriminalization didn’t increase use.
The gateway fear has focused mostly on youth. For example, newly-elected Maryland governor Larry Hogan announced that he is against legalization partly out of concern that “marijuana use would increase among young people.” Meanwhile, parents are concerned by recent research showing marijuana’s effect on the brain.
But fears of decriminalization resulting in increased use among youth haven’t been supported by research from countries where drugs were decriminalized. Nor has this trend been noted in studies of US states that legalized marijuana for medical or recreational purposes. For example, in an article published in the American Academy of Pediatrics, the authors found no evidence that young people had increased marijuana use in states that had legalized medical or recreational marijuana.
The worst impact on kids, according to these authors, was the potential for criminal prosecution.
A gateway to jail
Studies consistently find that the traumatic experience of being arrested and incarcerated for marijuana possession is the most harmful aspect of marijuana among young people. Arrest for possession can result in devastating – often permanent – legal and social problems, especially for minority youth and low-income families.
According to studies by the ACLU, nearly half of all drug arrests were for marijuana possession, and the majority of those arrested were African American. In some states, African Americans were more than eight times more likely to be arrested for marijuana than whites.
Unfortunately, marijuana legalization has not changed arrests and incarceration disparities for minorities. While African Americans have always been over-represented for drug arrests and incarceration, new research shows African Americans are more likely to be arrested for marijuana possession after marijuana reform than all other races were before marijuana policy reform. Although in some states, decriminalization makes possession a “noncriminal” offense, it can still be illegal and can result in an arrest, court appearance and stiff fines.
Marijuana as a gateway – out of hard drugs
On the periphery of the marijuana-as-gateway-drug debates are studies showing marijuana as beneficial for the treatment of opiate addicts.
These have been largely ignored. However, now that marijuana has become legal for medical purposes in some states, new research offers substantial findings that can’t be dismissed.
If anything, marijuana can work as a gateway out of hard drug use – an exit strategy that needs to be studied and, possibly, implemented at the policy level.
It’s time to move beyond marijuana as a gateway drug and start to study its use as treatment for the deadly, addictive and socially devastating drugs.
In recent years, hundreds of new synthetic recreational drugs have emerged – drugs that neither the general public nor the scientific community know very much about. Many of these new synthetic drugs – often referred to as “legal highs” – are dangerous and continue to lead to poisonings throughout the US and the rest of the world.
These drugs provide similar highs to other, more well-known drugs, like marijuana and cocaine. Many are still legal and others have only recently become illegal.
So why would people use these potentially harmful new drugs?
Drug users in the US have a lot to fear. Users of various drugs have to worry that the products they are using may be adulterated. Many must worry about unintentional poisonings, and (depending on the drug) addiction, as well.
But one of the biggest fears has nothing to do with safety or addiction. With illegal drugs, you are at risk for arrest. A drug-related arrest can prevent an individual from getting a good job, or from obtaining school loans or housing. The stigma associated with being a drug user can also serve as a major disruption to one’s life. A lot of people want to use or sell drugs, but fear repercussions. And that makes using or selling “legal highs” seem like a more attractive option.
But “legal,” in this case, doesn’t mean safe or regulated. Legal synthetic drugs are usually so new that laws to prohibit their use simply don’t (yet) exist. Even though they may be “legal,” these drugs have not gone through safety testing and it’s hard to know what you’re getting, or even where it’s coming from.
Spice, K2 and Scooby Doo – synthetic marijuana
Synthetic cannabinoids (hereafter referred to simply as “synthetic marijuana”), are the most prevalent of these new drugs in the US. Cannabinoids are natural compounds in marijuana that act on specific receptors in the brain. THC, the main psychoactive compound in marijuana, is the cannabinoid largely responsible for getting users high. Synthetic cannabinoids mimic the effects of the natural cannabinoids in marijuana, but have been reported to be much stronger and much more unpleasant than real marijuana.
Synthetic marijuana users rarely know what to expect because the products consist of untested research chemicals sprayed on an herbal mixture. It can be hard to know exactly where these drugs come from – but at least some are coming out of unregulated labs overseas. There are many compounds, mixtures and brands available and they aren’t very difficult to find. They’re widely available over the internet and also sold in some head shops throughout the US. Products come in catchy packaging under popular names such as Spice, K2 and Scooby Doo, and may be particularly appealing to young people. While some compounds are now illegal, they still remain available, and new synthetic (legal) compounds quickly emerge to take their place.
Synthetic marijuana use has been associated with tens of thousands of poisonings throughout the US. Alarmingly, results from my study published earlier this week suggest that between 2011 and 2013, one in ten US high school seniors reported using synthetic marijuana in the last year. In fact, a couple of years ago synthetic marijuana was the second-most prevalent drug used by teens (after real marijuana). However, use has begun to decrease since 2014.
Synthetic marijuana isn’t the only new drug out there
New synthetic drugs are beginning to pop up everywhere. You might have heard of “bath salts,” which are compounds or mixtures of synthetic drugs like the stimulants mephedrone and methylone. New drugs such as bath salts are often sold over the internet with users informed that they are “not for human consumption.” Despite extensive media attention, (intentional) use is not very prevalent.
Currently only about one out of a hundred high school seniors have reported use in the last couple of years. However, unlike synthetic marijuana, which is usually used intentionally, bath salts are often used unintentionally. In recent years, bath salts have been showing up frequently in the drug Molly, which is supposed to be pure MDMA (Ecstasy).
As I’ve discussed in The Conversation and in The Independent, many Molly users in the US don’t know the purity of the product they are using. A lot of batches of Molly have little to no MDMA and users should be worried that their Molly contains more dangerous synthetic chemicals such as methylone. Despite decreasing prevalence in use, “Ecstasy”-related poisonings and deaths have increased in recent years, and it appears that this is a result, in part, of Molly being so adulterated with new synthetic drugs.
Testing synthetic drugs is difficult
It is difficult for users to test their drugs to ensure purity. Special tests are needed to determine which drug is which and testing tends to be very expensive. In fact, testing is so expensive and time-consuming that some autopsies of deaths related to use of new drugs are backlogged or do not include tests for all new synthetic drugs. Making things more dangerous for users, pill and powder testing at rave parties and festivals is discouraged because promoters worry that it will be viewed as condoning drug use or admitting that use is occurring at the party. So those likely to try these new drugs are often stuck gambling with their lives as it is so difficult to test their products.
These new drugs are created in response to our drug policy and new drugs will continue to emerge. It seems that whenever we’re able to push one drug down, a newer, more dangerous synthetic drug, pops up to take its place.
E-cigarettes and other vaping products are on track to out-sell cigarettes by the end of 2023. And more and more young people are trying e-cigarettes. So what do you need to know about them? Are they less harmful than using cigarettes or other burned tobacco products?
What are e-cigarettes?
First, they are not burned tobacco products. Most often, they contain nicotine solutions that are heated to make a vapor (hence the terms vape or vaping), and they’re usually powered by batteries. Some look like cigarettes and others can resemble flashlights. The first e-cigarettes were not produced by cigarette companies, but the cigarette companies have gotten into the business. E-cigarette and vaping products are available in specialty stores and convenience stores around the US with varying restrictions on purchase by youth under 18.
E-cigarettes don’t necessarily contain nicotine. Some popular products contain little or no nicotine and levels can vary from brand to brand. And nicotine isn’t always the reason someone might try e-cigarettes. In Canada – where nicotine-containing e-cigarettes are not approved, but still widely available – only 38% of adult cigarette smokers who also use e-cigarettes “always use nicotine” and 30% “sometime use nicotine” when vaping. And only 4% of those who never smoked tobacco reported using nicotine when vaping.
Why do young people use e-cigarettes?
A 2014 national high school survey finds more monthly vapers than monthly smokers: 17% of US 12th-grade students report using e-cigarettes in the past 30 days compared to 14% for tobacco cigarettes. We also know that patterns of infrequent, non-daily use of various tobacco and nicotine products may be increasing among young people. But trying e-cigarettes does not automatically lead to daily use.
Young people might also be influenced to try e-cigarettes because of how they are priced and promoted. They can be cheaper than traditional cigarettes and may be perceived as safer. Other features, like flavors can also supportuse in all age groups.
As e-cigarettes become more popular and more visible, young people will start trying and using these products. And because products keep changing, they will often try different kinds of e-cigarettes.
Youth is a time when individuals experiment with and get into trouble with psychoactive substances, including nicotine-containing e-cigarettes. In 2014, 44.4% of 12th-graders had ever used marijuana/hashish, and 35.1% had used in the past year; 41.4% reported being drunk in the past year. Users of one type of psychoactive substance are more likely to use others, like caffeine, alcohol, nicotine, THC or prescription drugs.
Is vaping safer than smoking?
The best evidence to date shows that using e-cigarettes is very dramatically less dangerous than cigarette smoking. Death from all causes within the ages of 25 to 79 is three times higher for smokers than never smokers. Compared to smoking, long-term health effects of e-cigarettes have been judged as likely “much less, if at all, harmful to users or bystanders.”
The 2014 Surgeon-General Report concluded that “The burden of death and disease from tobacco use in the United States is overwhelmingly caused by cigarettes and other burned tobacco products; rapid elimination of their use will dramatically reduce this burden.”
Recent reports suggest that vapers should be cautioned about how they use high-voltage devices because they can produce high levels of the carcinogen formaldehyde. But that, however, is not one of the common ways people use e-cigarettes. High voltage devices and long puffs can produce a bad taste that is avoided.
Burned cigarettes contain many carcinogens: the FDA lists 79 “harmful or potentially harmful” carcinogens in tobacco products and tobacco smoke.
Keep in mind that reports of a product being “not safe” in some way does not necessarily mean that it cannot overall be much safer than another product.
Are e-cigarettes a gateway drug?
The specter of some drugs being gateways to more dangerous drugs has preoccupied drug policy, and this is no different when it comes to tobacco products. E-cigarettes have been feared as possible gateways to cigarettes. If vaping has been acting largely as a gateway to cigarettes, one would expect to see more cigarette smoking with the rise in vaping. This has not happened. Smoking has continued to decline. Cigarette smoking by young people is the most powerful cause of smoking by adults.
In a broad sense, the world is full of products that can look like gateway products. The use of BMX bikes on dirt tracks by children could be gateways to the use of motorcycle dirt bikes by adults. But do the products cause the linkage or are individual tendencies more responsible for associations?
Much research on drug gateways supports a “common liability model” more than drug-based causal models. The Common Liability Model holds that characteristics (for example, liking to take risks) within individuals can be responsible for drug-use associations.
No matter whether you think (a) that trying of an e-cigarette is a causal gateway to later smoking that would not have otherwise happened or (b) that those who are more likely to try cigarettes are more likely to try e-cigarettes, once products become available to users, how these products are marketed influence which products are preferred. What is said and done about vaping can promote gateways to cigarettes. If you show more concern about vaping than smoking or if you downplay the deadly risks of smoking, you encourage young people to switch to cigarettes.
The policies that allow certain substances, like alcohol, tobacco and psychoactive substances, to be used quite freely by adults usually include prohibitions on use or purchase by youth. Without such policies, there might be even more experimentation by youth with these products. Prohibitions on sale of vaping products to youth should be supported.
What should you do if your teen smokes?
If you are faced with committed teenage smokers (who are probably also using other prohibited substances like drugs or alcohol), perhaps the best you can do is foster switching to e-cigarettes. Of course, do explore their interest in getting help with quitting smoking from quit-lines. For less-involved users of e-cigarettes who do not smoke regular cigarettes, encourage that regular use be avoided and that nicotine use be limited as much as possible.
Telling a teenager that vaping is just as bad for you as smoking or that e-cigs are worse than tobacco cigarettes could push them toward cigarettes and is not justified. It makes more sense to tell a young person that it is much better for their health if they stay away from tobacco cigarettes or cigarette-like tobacco cigars completely.
If you have teenagers who already both smoke and vape, encourage that they work to avoid cigarettes completely, and vaping could help them do so.
At present, cannabis is fully legalized in Colorado and Washington and will soon be fully legalized in Oregon and Alaska. Additionally, medical cannabis is legal in 23 states. The writing is on the wall that more and more states are going to legalize cannabis in various ways and that access will become easier and easier. In the face of this reality, two big questions arise: will cannabis usage skyrocket? Will addiction rates go through the roof?
The answer to both is probably not.
Is marijuana addictive?
Before we even get to the question about possible increased rates of addiction, some people will object because they don’t think marijuana is addictive.
Because the symptoms of marijuana withdrawal are somewhat mild compared to other drugs, people often believe that marijuana is not addictive. After all, those who quit generally experience fairly subtle physiological signs of withdrawal – a mildly elevated pulse, irritability and cravings. These symptoms are much less obvious or powerful than those seen when someone addicted to alcohol, painkillers, or tranquilizers suddenly stops using. When quitting one of these drugs, individuals in withdrawal are often visibly and dramatically uncomfortable. They can have very high pulse rates and blood pressures, can hallucinate and in worst cases have seizures and even die.
Just because the signs of cannabis withdrawal are comparatively mild, though, doesn’t mean it isn’t addictive.
Being addicted to something is more than simply being physically dependent on a drug and experiencing physiological effects if it’s suddenly stopped. “Addiction” refers to behaviors that are compulsive and partially out of control or worse. These behaviors can often escalate in severity and intensity. People can be addicted to gambling, abusing alcohol or other drugs, or other kinds of behavior.
Think about it this way: those who take pain medications around the clock for legitimate health reasons are not addicted, even if they are physiologically dependent on those drugs. Unless someone is physically dependent on a drug and it is also causing problems in that person’s life, they don’t meet the clinical definition of addiction. If the drug dominates their daily existence, causes them to engage in dangerous behaviors in order to procure the drug, or they’re spiraling out of control, then they definitely have a problem and might well be addicted.
The younger someone is when they use marijuana for the first time, the more likely they are to become addicted to it later in life. So those who started using marijuana in adolescence are much more likely to become addicted to marijuana than others and to experience withdrawal symptoms if they suddenly stop. They are also more likely experience depression and anxiety. This is because our brains continue to develop into our mid- to late-20s.
Will legalization increase addiction?
So what, if anything, does all of this mean for legalization? Does the fact that cannabis is increasingly legal mean that addiction rates are going to spike and related issues – such as lower IQs and higher rates of marijuana addiction – are also going to jump?
I believe the answer is no. Despite these legitimate concerns, thus far there are no compelling data to suggest that drug use has increased in Colorado where recreational cannabis is currently legal. Even though it’s only recently that Colorado legalized marijuana, I don’t expect this to change going forward.
A large study found that rates of cannabis use among teenagers in states that legalized medical marijuana did not increase. And since Colorado fully legalized cannabis in 2013, the early reports show that rates of cannabis consumption among teens have continued to decline, which is part of a nation-wide trend.
Additionally, we have an example of a country where drugs were decriminalized over a decade ago. Portugal decriminalized drug use in 2001. Drug users are not punished for their offense when found to possess drugs, but instead are offered access to treatment and rehab. The result: a decade later, drug abuse was cut in half in Portugal. Specifically among Portuguese teens in grades 10 through 12, lifetime prevalence rates of marijuana use decreased from 26% in 2001 to 19% in 2006.
This is not to say that drugs of abuse in general, and cannabis in particular, are benign. Indeed, they are addictive and can harm brain development. But decriminalizing or legalizing drug use makes sense because it reduces crime almost immediately, frees up police for more serious matters and will likely not lead to higher rates of use.




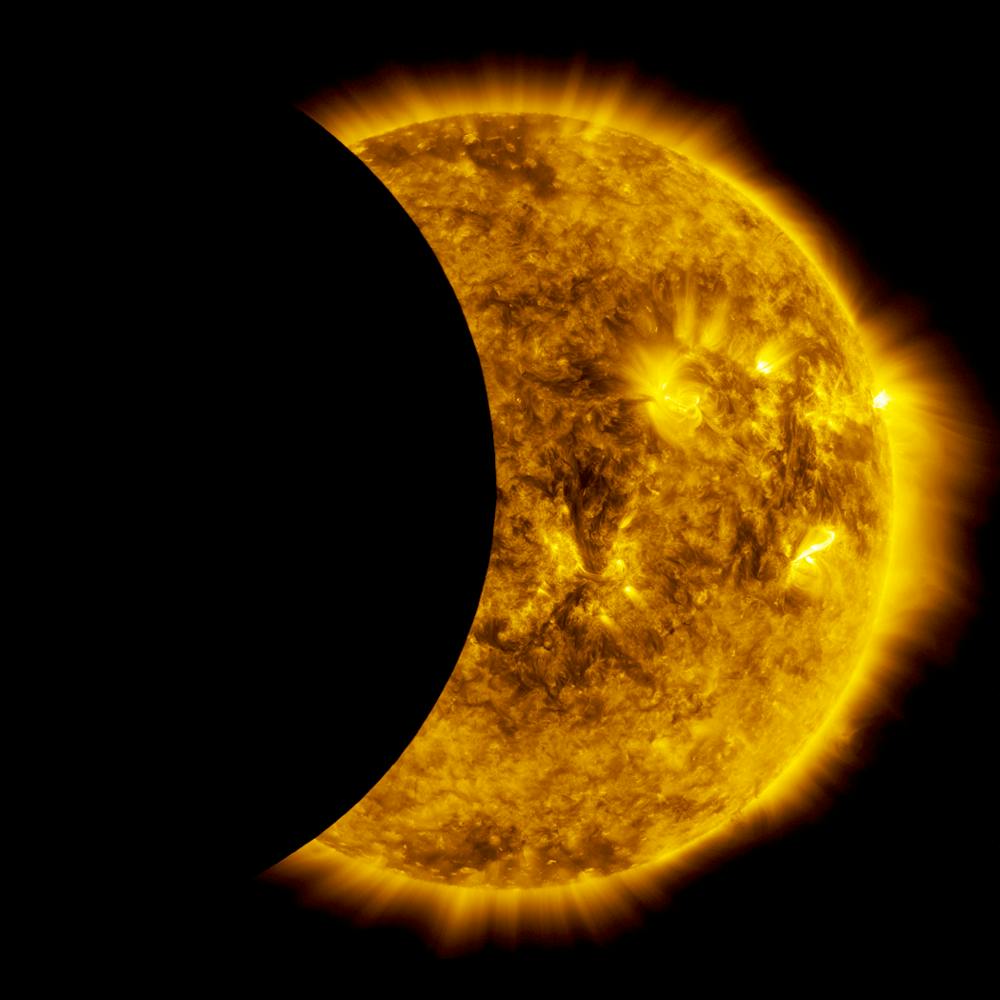

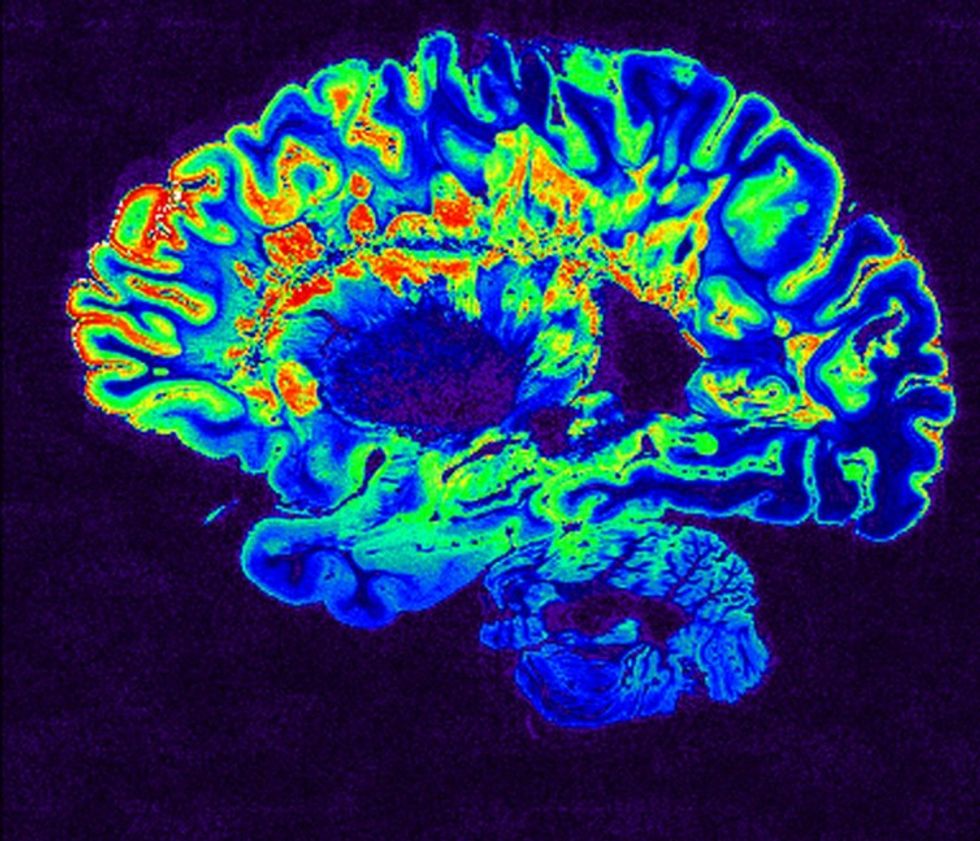





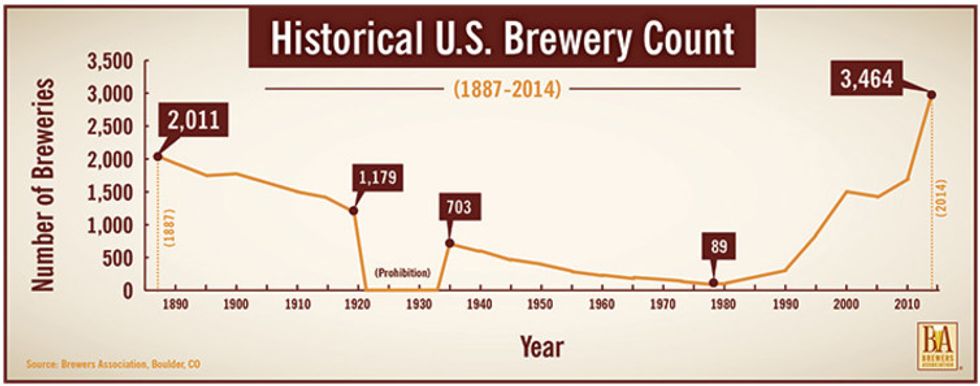






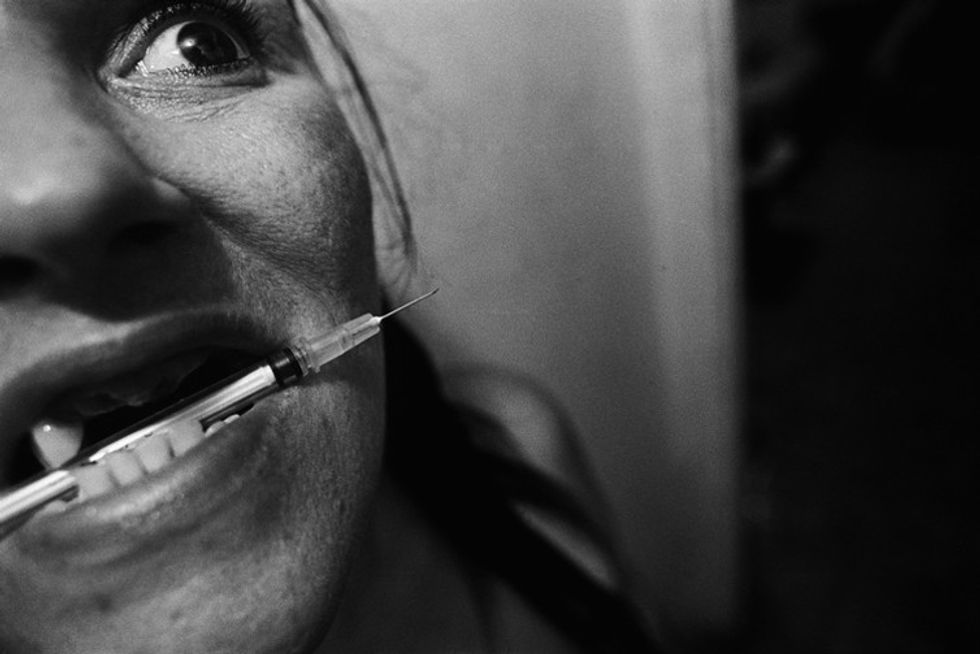























{kind=link}
{kind=link}
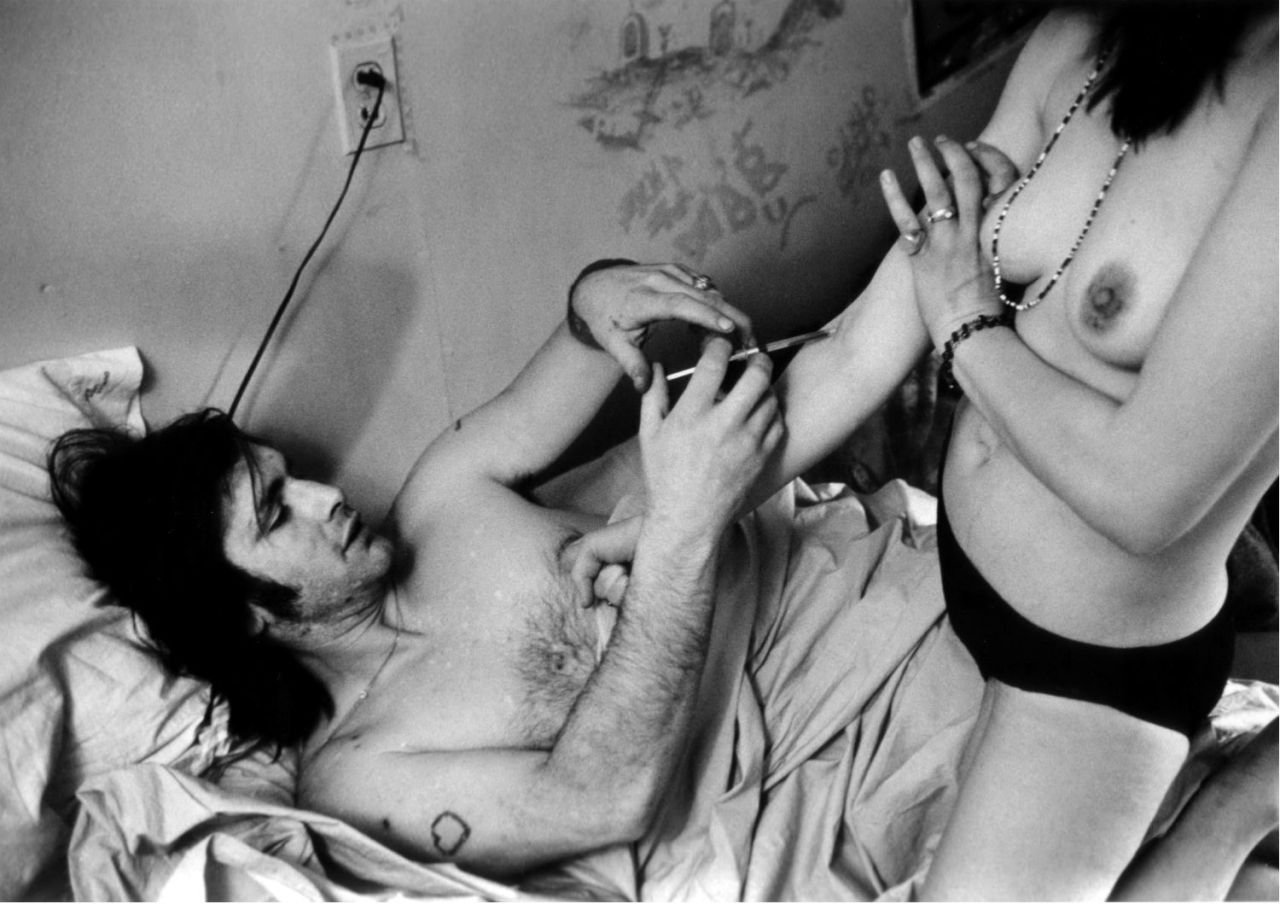{kind=link}
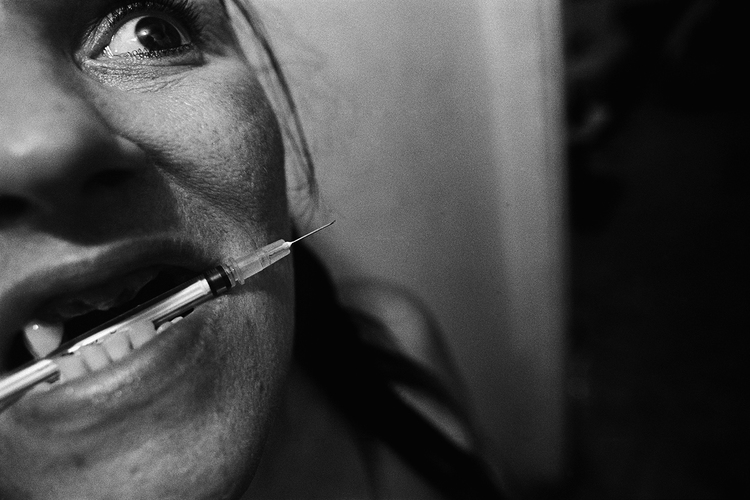{kind=link}
{kind=link}
{kind=link}